
Part A – Excellence in commissioning and partnership working
1. Excellence in commissioning and partnership working
1.1 Introduction
To support commissioners, NHS England has reviewed and updated the 2018 version of the policy book and several additions and amendments.
The Health and Care Act 2022 gained royal assent on 28 April 2022. It has amended the NHS Act 2006 in several ways including:
- formally established integrated care boards (ICBs at the same time as abolishing Clinical Commissioning Groups (CCGs); and,
- introduced power to establish a new NHS Provider Selection Regime (PSR). To support implementation of the PSR , which came into force on 1 January 2024, NHS England has published its statutory guidance to support implementation of the PSR regulations and set out what relevant authorities must do to comply with them. The statutory guidance sits alongside the PSR regulations supporting relevant authorities to understand and apply the PSR.
The amendments to the NHS Act have also facilitated a change to who commissions primary and secondary dental services. From April 2023 NHS England delegated responsibility for commissioning primary and secondary dental services. The Delegation Agreement and related guidance set out the responsibilities of ICBs and NHS England. The definition and reference to ‘the Commissioner’ within this revised policy book is the responsible commissioner for primary care dental services and includes NHS England and ICBs as appropriate.
This policy and guidance manual has been updated to reflect the changing landscape in primary care commissioning and provides commissioners of dental services with the context, information, and tools to commission and manage dental contracts.
This policy has also been reviewed and refined in light of:
- feedback from users
- engagement with stakeholders
- contractual and regulatory changes
This policy book provides new and revised policies to support a consistent and compliant approach to primary care commissioning across England and identifies sections which describe mandatory functions (i.e. those absolutely defined in legislation) versus those which are provided as guidance or best practice.
The policy booklet has been divided into three parts (A-D). All supporting documents and templates are provided as appendices in the accompanying document.
Part A – Excellence in commissioning and partnership working
- Introduction with abbreviations and acronyms – An existing chapter with minor updates
- General duties of NHS England (including addressing health inequalities)
Part B – General contract management
- Which dental contract when?
- Contract variations – an existing chapter that has been updated to remove reference to the 16 hour rule
- Body corporates – variations and incorporations – an existing chapter that has been updated to remove reference to Public Contracts Regulations 2015 (PCR2015)
- Changes to services and finance – an existing chapter that has been updated to include reference to flexible commissioning
- Managing a PDS Contractor’s right to a GDS contract
- Financial recovery and reconciliation – an existing chapter that has been updated with reference to persistent underperformance
- Orthodontics
- Contract breaches
- Contract terminations and sanctions – an existing chapter that has been updated to remove requirement for commissioners to submit a template notice return
- Death of a contractor
- Managing disputes
- Adverse events
- Practice closedown
- Practice NHS.UK profile
- Provision of occupational health services
NHS England recognises the pace and scale of change in Primary Dental Care commissioning, service delivery and redesign. As such it is committed to reviewing this policy and guidance regularly, to ensure it supports the commitments set out in the NHS Long Term Plan and with changes in legislation and regulation.
Users of this policy book are advised this is a controlled document and the most up to date version should always be used. That is, the version which is published on NHS England’s website: NHS England » Policy book for primary dental services.
Provisions during times of national emergencies
This policy book is provided to commissioners to support their commissioning and contractual management responsibilities on a normal basis.
It is recognised that there may be occasions when national challenges require commissioners to work more flexibly. Statutory duties will remain along with the responsibilities for quality and safety, but commissioners may need to pause some standard processes. This will be informed by emergency legislation or policy requirements which may be in place.
1.2 Transitional arrangements
This policy book replaces all previous versions. In addition, we have incorporated some other related policy and guidance that has been published by NHS England as standalone documents since the original ‘Policy Book’ was published in December 2016.
The processes and procedures set out must be followed where a matter arises after the date of the publication of this updated policy book.
Where a matter arose prior to the publication of this updated policy book (and the parties are therefore following a previous policy) the parties should continue to follow that previous policy as this would have been the expectation of the parties.
Parties following a previous policy should consider switching to the relevant policy set out in this policy book if there is a natural transitional point in the matter and provided all parties agree.
1.3 Abbreviations and acronyms
The following abbreviations and acronyms are used in the dental policies:
- CQC – Care Quality Commission
- GDS – general dental services
- GDS Regulations – The National Health Service (General Dental Services Contracts) Regulations 2015
- GDS SFE – General Dental Services Statement of Financial Entitlements Direction 2013
- GDP – general dental practitioner
- HWB – health and wellbeing boards
- ICS – integrated care system
- ICB – integrated care board
- LDC – local dental committee
- MCP – multi-speciality community provider
- NACV – negotiated annual contract value
- NBM – new business models
- NCM – new care models
- NHS Act – National Health Service Act 2006
- NHSBSA – NHS Business Services Authority
- NHS R – NHS Resolution
- OH – occupational health
- PACS – primary and acute care systems
- PCSE – Primary Care Support England (delivered by Capita on behalf of NHS England
- PDS – personal dental services
- PDS Regulations – The National Health Service (Personal Dental Services Agreements) Regulations 2015
- PSR – provider selection regime
- SOs – standing orders
- SFIs – standing financial instructions
- TUPE – Transfer of Undertakings (Protection of Employment) Regulations 2006
- UDA – unit of dental activity
- UOA – unit of orthodontic activity
2. General duties of NHS England (including addressing health inequalities)
2.1 Introduction
ICBs carrying out commissioning under delegated authority do so on behalf of NHS England. ICBs will need to comply with their own legal duties as well as ensuring that they commission in such a manner as to ensure NHS England’s compliance with its statutory duties.
There are many general duties on commissioners. It is important that decision-makers are familiar with all of these duties because if a duty has not been complied with when a decision is taken, that decision can be challenged in the courts on the grounds that it is unlawful.
This guidance looks at the general duties that commissioners are required to comply that are most applicable to primary care, providing examples to illustrate how they might affect decision-making.
The full wording from the legislation is provided at Annex 2.1. This guidance goes on to look at each of the duties in more detail.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 2.1: Extracts from legislation
2.2 Equality and health inequalities duties
This section considers equality and health inequality duties. First, the duties under the Equality Act 2010 are considered followed by the other health inequality-related duties.
2.2.1 Equality Act 2010
Commissioners have both general and specific equality related duties under the Equality Act 2010. The general duty can be found in section 149 of the Equality Act 2010. It is known as the public sector equality duty or the PSED. The specific duties are imposed on commissioners by secondary legislation, namely the Equality Act 2010 (Specific Duties and Public Authorities) Regulations 2017. Further details on both the PSED and the 2017 Regulations are provided in the sections below.
The duty to have regard to the PSED will arise when commissioners are exercising their functions. A Commissioner will be open to legal challenge if the commissioner is unable to demonstrate how it had regard to the PSED when publishing guidance or policies or making decisions. A failure to comply with the prescribed duties outlined in the 2017 Regulations will also be unlawful.
2.2.2 The protected characteristics
The Equality Act 2010 prohibits unlawful discrimination in the provision of services (including healthcare services) on the basis of “protected characteristics”. The protected characteristics are:
- age
- disability
- gender reassignment
- marriage and civil partnership
- pregnancy and maternity
- race
- religion or belief (which can include an absence of belief)
- sex
- sexual orientation
Unlawful discrimination can also occur if a person is put at a disadvantage because of a combination of these factors.
2.2.3 Unlawful discrimination
There are broadly four types of discrimination in the provision of services that are unlawful under the Equality Act:
- Direct discrimination occurs where services are not available to someone because they are, for example: not married, over 35, a woman. Apart from a few limited exceptions, direct discrimination will always be unlawful, unless it is on the grounds of age and the discrimination is a proportionate means of achieving a legitimate aim.
- Indirect discrimination occurs when commissioners apply a policy, criterion, or practice equally to everybody, but which has a disproportionate negative impact on one of the groups of people sharing a protected characteristic, and where the complainant cannot comply. The classic example is a height requirement, which is likely to exclude a much greater proportion of women than men because women are on average shorter than men. Requirements that require people to behave in a certain way will amount to indirect discrimination if compliance is not consistent with reasonable expectations of behaviour. For example, a requirement not to wear a head covering would be indirectly discriminatory on the grounds of religion, even though followers of religions which require a head covering are physically able to remove it. Indirect discrimination is not unlawful if it is a proportionate means of achieving a legitimate aim.
- Disability discrimination occurs if a person is treated unfavourably because of something “arising in consequence of their disability”. This captures discrimination that occurs not because of a person’s disability per se (e.g. a person has multiple sclerosis) but because of the behaviour caused by the disability (e.g. use of a wheelchair). So, an inability of someone with multiple sclerosis to access services when using their wheelchair could be an instance of disability discrimination.
- Disability discrimination is not unlawful if it is a proportionate means of achieving a legitimate aim.
- A failure to make “reasonable adjustments” for people with disabilities who are put at a substantial disadvantage by a practice or physical feature. The duty also requires bodies to put an “auxiliary aid” in place where this would remove a substantial disadvantage (e.g. a hearing aid induction loop). The duty to make reasonable adjustments might require NHS England or an ICB to make consultation materials available in braille. However, some care is needed here. People with disabilities have a right to access services in broadly the same way as people without disabilities, so far as is reasonable. Offering a telephone consultation to a wheelchair using patient who is prevented from accessing a clinic by steps may in fact be unlawful discrimination rather than a reasonable adjustment. The wheelchair user should be able to access services in broadly the same way as others i.e. by attending practice premises for a consultation.
- (Unlawful discrimination is also prohibited in the field of employment and other areas, but these are not covered in this)
2.2.4 Public sector equality duty
The Equality Act 2010 requires commissioners to have “due regard” to the need to:
- eliminate discrimination that is unlawful under the Act
- advance equality of opportunity between people who share a protected characteristic and people who do not share it
- foster good relations between persons who share a protected characteristic and persons who do not share it
These objectives are often referred to as the “three aims” of the PSED. The aims are amended for the protected characteristic of marriage and civil partnership. commissioners must have due regard to eliminate unlawful discrimination based on marriage and civil partnership (the first aim). However, they are not required to have due regard to the need to advance equality of opportunity or foster good relations in relation to marriage and civil partnership (the second and third aims).
Compliance with the three aims of the PSED can require a Commissioner to take positive steps to reduce inequalities. In this regard the Act permits treating some people more favourably than others but not if this amounts to unlawful discrimination (what is meant by unlawful discrimination is considered below). The PSED has been used successfully on many occasions to challenge changes to services.
This means that a Commissioner has a duty to help eliminate any unlawful discrimination practised by the providers of primary care e.g. through requiring premises to be accessible. Failing to use its negotiating power to secure such changes could be seen as a breach by a Commissioner of the PSED, as well as a breach of the non-discrimination rules by the service provider.
From 1 August 2016 onwards, all organisations that provide NHS care and/or publicly funded adult social care are legally required to have regard to the Accessible Information Standard (DCB1605 Accessible Information). The standard sets out a specific, consistent approach to identifying, recording, flagging, sharing, and meeting the information and communication support needs of patients with a disability, impairment, or sensory loss.
Example
After a site visit the Commissioner becomes aware that consulting rooms in a dental surgery are no longer accessible to those with limited mobility as they have been moved upstairs. The Commissioner decides that as there are no downstairs consulting rooms and there is no lift or stair lift, this is a breach of the practice’s duty to make reasonable adjustments under the Equality Act. This in turn is a breach of the practice’s duty under its contract with the Commissioner to comply with legislation. In order to comply with the PSED the Commissioner takes steps to ensure that the practice complies with its Equality Act duties by raising the issue informally and issuing a Breach Notice if the problem is not remedied.
Example
A hearing-impaired patient complains to the Commissioner about their experience with a local (NHS commissioned) provider. The patient was unable to communicate effectively with the provider because of their hearing impairment. When the patient suggested that the provider obtain a sign language interpreter to translate for them this was refused.
It is likely that the provider will be in breach of their obligations under the Equality Act 2010 to make reasonable adjustments. In order to comply with the PSED the Commissioner takes steps to investigate and take enforcement action if needed.
Carrying out appropriate equality and health inequalities impact assessments (EHIAs) is usually critical to demonstrating compliance with the PSED, although they are not as such a legal requirement. This is because if there is no assessment of the impact of a possible change on groups with protected characteristics, it is very difficult to argue that the Commissioner had the impact properly in mind when it made its decision. This is the case even if the impact on protected groups is minimal.
It is not always easy to assess equality impact. A robust service user involvement exercise will help the Commissioner identify any issues. It is advisable to ask question(s) directly aimed at equalities issues. In many cases it is advisable to take special steps to reach seldom heard groups affected by the decisions (e.g. by working with local voluntary, community and faith sector groups and holding meetings in community venues). The more likely a decision is to disproportionately affect a protected group, the more important it is to get feedback from that group about the decision. Undertaking a literature search can also be helpful to see what evidence is available. NHS England’s Equality and Health Inequalities Unit has a Resource Hub with information.
The PSED means that NHS England and ICBs must consider equalities issues when making decisions. In some cases, there may be a solution that causes less disadvantage to a protected group but for other reasons is undesirable. In these situations, it is important to acknowledge the disadvantage caused and be clear about why the decision was taken. This may include outlining costs concerns. It also makes sense to monitor the situation e.g. does the demographic of service users change because of the decision and timetable a formal review in e.g. a year’s time.
There are a few themes arising from the cases we have seen so far on the application of the PSED (and similar duties in previous legislation):
- a need to explicitly recognise that the PSED applies, and equalities issues need to be considered
- the duty is an ongoing one – to be considered at all stages of decision-making not just at the end
- a need to be clear about the factors driving a decision, even if these are unpalatable e.g. budgetary pressures
- a need to analyse in some detail the impact of a proposed policy or decision so that the public authority has a clear idea of who is affected and how. Statements of impact need to be supported by evidence where possible
- if a decision is made that will impact negatively on a protected group, that should be acknowledged, and the rationale explained
- there should be a detailed consideration as to how any negative impact of the decision could be mitigated. If the steps identified are not practicable, this should be explained
- the duty must be complied with at the time of the decision. After the event reasoning is rarely allowed so a record should be made at the time about how equalities issues are being considered
Further guidance on the PSED can be found on NHS England’s Equality and Health Inequalities Unit Resource Hub.
Additionally, the Equality and Human Rights Commission publish a wealth of information.
Guidance on the PSED can also be found on the EHRC’s website.
2.2.5 The Equality Act 2010 Specific Duties
In addition to the PSED NHS England and ICBs are also required to comply with the specific duties contained in the Equality Act 2010 (Specific Duties and Public Authorities) Regulations 2017.
The 2017 Regulations came into force on 31 March 2017. The 2017 Regulations replace the first set of specific duty regulations made in 2011.
Amongst other things, the 2017 Regulations require commissioners to publish;
- equality objectives that should be achieved to comply with the PSED (Regulation 5). This must be completed by 30 March 2018 and the objectives need to be updated once every four years. Details of NHS England’s equality objectives have been published on the Resource Hub. Co-commissioners should ensure that they are familiar with NHS England’s equality objectives.
The Equality and Human Rights Commission can, under sections 31 and 32 of the Equality Act 2006, investigate and enforce a failure to comply with the PSED or the specific duties. Alternatively, a failure to comply with the general and specific duties could be challenged by way of judicial review. Such a claim could be brought by a person or group directly affected by a failure to comply with these duties.
2.2.6 Health Inequalities Duties and the NHS Act 2006
Under the NHS Act 2006, commissioners are required to have regard to the need to:
- reduce inequalities between persons with respect to their ability to access health services, and
- reduce health inequalities between patients with respect to the outcomes achieved for them by the provision of health service
When making decisions about primary care, particularly about service changes, decision-makers will need to bear in mind the impact on health inequalities. To do this the Commissioner will need data on existing health inequalities, and to consider whether its decision can be used to reduce these. A vast amount of data is available e.g. JNSA’s; e.g. Right Care packs to help commissioners identify health inequalities in their area.
The key point is that the commissioner should be able to demonstrate (through documentation, principally an EHIA) the impact a decision will have on health inequalities, this has been considered and is supported by relevant data and evidence. NHS England and Public Health England have made available several resources to assist organisations to find out about information, resources and action being taken to reduce health inequalities in England. Local Joint Strategic Needs Assessments (JSNA) prepared by local Health and Wellbeing Boards, indicators and NHS Right Care can be valuable sources of information about local health inequalities.
2.3 The Regard Duties
The “Have regard”, “act with a view to” or “promote” duties. These form a loose hierarchy of duties:
- the duty to have regard means that when taking actions, a certain thing must be considered
- the duty to promote means action must be taken that actually achieves an outcome. Additionally, it is possible to promote something by encouraging others to do it
- the duty to act with a view to means that action must be taken with a purpose in mind
In contrast to the Promotion Duties and the View to Duties, the Regard Duties apply to every action of a commissioner where it is carrying out its primary care functions, (except the duty will not normally apply to “private law” decisions that would be taken by any private sector organisation – making HR decisions, leasing estate etc.).
The PSED cases are the best guide that we have to how a court would interpret a Commissioner’s Regard Duties under the NHS Act. We can learn from these that:
- commissioners who take decisions must be made aware of their duty to have regard to the various issues outlined in the duties. Failure to do so will render the decision unlawful
- the Regard Duties must be fulfilled before and at the time that a particular decision is being considered. If they are not, any attempts to retrospectively justify a decision as consistent with the Regard Duties will not be enough to discharge them
- commissioners need to engage with the Regard Duties with rigour and with an open mind.
- it is good practice for the decision maker to make reference to the Regard Duties
- it is not possible for the commissioner to delegate the duties down to another organisation to comply with. They will always remain with NHS England. If NHS England acts through Contractors, it must ensure as necessary that they act consistently with the duties
- the Regard Duties are continuing ones that apply throughout decision-making. It is not enough to only “rubber stamp” a decision by reference to the Regard Duties at the end of a decision-making process. The Regard Duties need to be borne in mind throughout
- it is crucial to keep an adequate record of how the Regard Duties are considered. If records are not kept it will make it more difficult, evidentially, for NHS England to persuade a court that it has fulfilled the duties imposed
One key point to understand is that there is no obligation to achieve the object of the Regard Duties e.g. it is not unlawful not to eliminate health inequalities (although equally, if health inequalities persist and widen, that fact would need to inform consideration of the regard duty). Nor does the commissioner have the luxury of “pausing” the health service while it investigates health inequality or any other matter. The duties are to have regard, not to achieve perfection, and should be done pragmatically as a practical rather than an academic exercise.
2.3.1 Reduce health inequalities
Of the Regard Duties, the requirement to have regard to the need to:
- Promoting equality and addressing health inequalities are at the heart of NHS England’s values.
The commissioner has duties to:
- have regard to the need to reduce inequalities between persons in access to health services and the outcomes achieved (s. 13G and s.14Z35)
- exercise its functions with a view to securing that health services are provided in an integrated way and are integrated with health-related and social care services, where it considers that this would improve quality, reduce inequalities in access to those services or reduce inequalities in the outcomes achieved (s.13N and s.14Z42). Outcomes include the effectiveness of services, safety of services and the quality of experience undergone by patients
Lawyers advise that “have regard to the need to reduce” means health inequalities must be properly and seriously considered when making decisions or exercising functions, including balancing that need against any countervailing factors. Part of “having regard” includes accurate record keeping of how the need to reduce health inequalities has been considered when making decisions or exercising functions. The duty must be exercised with rigour and an open mind and should not materialise as an afterthought in the process of reaching a decision.
Commissioners must be able to demonstrate that:
- they are fully aware of the duty
- the duty was considered during the appropriate stages of work, from the beginning of the decision-making process and throughout
- the appropriate amount of weight has been given to factors which would reduce health inequalities in the decision-making process
- they have actively considered whether integration would reduce inequalities and act with a view to securing such integration where it would do so
- accurate records have been kept showing that the need to reduce health inequalities was taken into account throughout decision making processes
To be compliant with the legislation there should consistently be regard to the need to reduce inequalities when exercising their functions. This is likely to require considering:
- the impact on inequalities as part of all decision-making processes, and keeping a record of such processes
- which dimensions of inequality are relevant to their work and taking account of how inequalities could be reduced
2.3.2 Act with autonomy
NHS England has a duty to have regard to the desirability of allowing others in the healthcare system to act with autonomy and avoid imposing unnecessary burdens upon them, so far as this is consistent with the interests of the health service.
Example
NHS England is considering commissioning new primary care services in a particular area. When deciding what type of contract it wants to award (GDS, PDS or PDS+) NHS England should weigh in the balance the desirability of the extra autonomy a PDS or PDS+ contract offers.
2.3.3 Triple Aim Duty
The Health and Care Act 2022 introduced a new duty into the NHS Act 2006 known as the Triple Aim Duty (section 13NA and 14Z43). This requires NHS England and ICBs to have regard to all likely effects of decisions about the exercise of its functions. This duty requires, in particular, regard to all likely effects of the decision in relation to the health and well-being of the people in England, the quality of services provided to individuals for or in connection with the prevention, diagnosis or treatment of illness, and the efficient and sustainable use of resources. NHS England may publish guidance about the discharge of this duty.
2.3.4 Promote education and training
NHS England has a duty to have regard to the need to promote education and training of those working within (or intending to work within) the health service.
2.3.5 Impact in areas of Wales or Scotland
NHS England has a duty to have regard to the likely impact of commissioning decisions on healthcare delivered in areas of Wales or Scotland close to the border with England. This will clearly be relevant for those working in ICB teams that border Wales or Scotland. NHS England will also need to comply with the duty when making national strategic decisions about the delivery of primary care – that affect bordering areas as well as others.
Example
The commissioner is considering commissioning new primary care services for a town in England close to the border with Scotland. It is concerned that many of the local residents have difficulty in accessing local primary care services, the nearest practice being based over the border in Scotland. That provider is difficult to access by public transport and in the winter the short route is often impassable. To comply with its duty NHS England discusses the impact that commissioning services on the English side of the border will have on the Scottish border. It takes this impact into account when it makes its decision about the commissioning of services.
2.3.6 Compliance with net zero emission and other environmental targets
The Health and Care Act 2022 introduced a new duty into the NHS Act at 13ZC and 14Z44 that requires NHS England and ICBs to have regard to the need to contribute towards compliance with section 1 of the Climate Change Act 2008 (UK net zero emissions target) and section 5 of the Environment Act 2021 (environmental targets) and adapt to any current or predicted impacts of climate change identified in the most recent report under section 56 of the Climate Change Act 2008. NHS England may publish guidance about the discharge of this duty.
2.4 The promote duties
These are:
- the duty to promote awareness of the NHS Constitution among patients, staff, and members of the public (see section 13C(1)(b) and 14Z32(b) of the NHS Act 2006)
- the duty to promote the involvement of patients and carers in decisions about their own care (see section 13H and 14Z36 of the NHS Act 2006)
- the duty to promote innovation in the health service (see section 13K and 14Z39 of the NHS Act 2006)
- the duty to promote research and the use of research on matters relevant to the health service (see section 13L and 14Z40 of the NHS Act 2006)
A decision which is positively contrary to achieving the relevant outcome might breach a promote duty unless there was some compelling reason to adopt it. In this situation, the commissioner should seek legal advice for further guidance.
Additionally, some decisions will be obvious opportunities where e.g. patient involvement could easily be promoted. In such cases the safest course of action is to ensure that this is done.
To meet the duty a commissioner does not have to do everything itself – a commissioner can be more innovative, improve its use of research data etc. It can meet the duty by encouraging other people to do things.
2.5 The view to duties
The “View to Duties” are:
- the duty to act with a view to delivering services in a way that promotes the NHS constitution (see section 13C(1)(a) of the NHS Act 2006).
- the duty to act with a view to securing continuous improvement in the quality of services in health and public health services (see section 13E of the NHS Act 2006).
- the duty to act with a view to enabling patients to make choices about their care (see section 13I of the NHS Act 2006).
- the duty to exercise its functions with a view to securing that health services are provided in an integrated way where it considers that this would:
- Improve the quality of those services (including the outcomes that are achieved from their provision)
- Reduce inequalities between persons with respect to their ability to access those services
- Reduce inequalities between persons with respect to the outcomes achieved for them by the provision of those services
In many ways the considerations for these duties and the Promote Duties are the same. One difference is that while a Promote Duty can be met by encouraging others to achieve it (e.g. encouraging GP practices to make better use of telehealth devices), with the View to Duties the actions must be carried out by the commissioner.
The View to Duties is less onerous than the Promote Duties because they do not require the commissioner to achieve a particular outcome (although that would be desirable) only to do something that aims to achieve it. This contrasts with the Promote Duties, which require an outcome to be achieved.
The View to Duties is most likely to affect strategic decisions taken at directorate level within NHS England. Provided the commissioner can show that within the totality of its activities there has been significant action taken with the intention of achieving the outcomes that the commissioner is required to have a view to, the duty is discharged.
As with the Promote Duties, decision-makers on the ground should be wary of doing something which actively goes against one of the goals set out in the View to Duties. In this situation, if the decision is being made by NHS England or by an ICB, the commissioner should seek legal advice for further guidance. Also, if there is a clear opportunity to help deliver one of the View To objectives, it is best to take it.
2.6 The involvement duty
1.6.1 Overview
NHS England and ICBs have a statutory duty to ‘make arrangements’ to involve the public in the commissioning services for NHS patients (Section 13Q and section 14Z45 of the NHS Act 2006).
Section 13Q and 14Z45 applies to:
- the planning of commissioning arrangements
- the development and consideration of any proposals that would impact on the way services are delivered to individuals or the range of services available to them
- decisions that would impact on the way services are delivered to individuals or the range of services available to them
NHS England has published guidance on involving the public in the Guidance document “Working in Partnership with people and communities: Statutory Guidance”.
2.7 Duty to act fairly and reasonably
Commissioners have a duty to act fairly and reasonably when making its decisions. These duties come from case law that applies to all public bodies.
2.7.1 Acting fairly
Normally, to act fairly a commissioner will need to act in accordance with its own
policies. and relevant policies published by NHS England. For ICBs co-commissioning under delegated authority from NHS England, this will include NHS England policies concerned with the commissioning of primary care. A commissioner can depart from guidance if there is good reason to do so. In this scenario the commissioner will need to explain the situation fully to the people and organisations affected and give them a chance to provide their views on the procedure to be followed. This will include why it wants to depart from the usual policy and what it will do instead.
Commissioners also need to be careful about keeping to promises made to Contractors or the public; for example, that there will be a public consultation before any final decision is made on closing a particular dental practice. It is sometimes (but not always) possible depart from such promises. Therefore, care should be taken about giving any clear commitments to a particular course of action until the commissioner is sure that it is what it wants to do. If a commissioner is considering departing from a commitment it has given to do a particular thing or follow a particular type of process, then, if the decision is being made by NHS England or by a ICB co-commissioning under delegated authority from NHS England, the commissioner should seek legal advice for further guidance.
It is also important to act proportionately, considering any adverse impact on patients and/or Contractors.
2.7.2 Acting reasonably
The commissioner must take all relevant factors into account when making its decisions and exclude irrelevant factors. It is up to the commissioner how much weight it gives competing considerations and may give a factor no weight at all. The key point is that all the relevant factors are identified and documented.
Example
The commissioner must decide whether to approve a practice’s application to stop opening on Wednesday evening and open on Saturday morning instead. The practice is based in an area with a high Jewish population. Relevant factors in this decision include whether services will become more or less accessible as a result of the change, any adverse impact on people with protected characteristics (is the Jewish population disadvantaged as Saturday falls on the Jewish rest day?) and any costs implications for the commissioner. An example of an irrelevant factor is that the commissioner has been promised some good publicity by the practice if it agrees to the change.
The reasons for the Commissioner’s decisions also need to “stack up”. It is important for the commissioner to document its reasons for a decision as the commissioner needs not only to act reasonably but be able to show that it has acted reasonably by reference to contemporaneous documents. This means that particularly where a controversial decision is being made the thinking behind the decision needs to be carefully documented.
2.8 The duty to obtain advice
A commissioner has a duty to “obtain appropriate advice” from persons with a broad range of professional expertise (in respect of NHS England, see section 13J of the NHS Act; and, in respect of ICBs, see section 14Z38 of the NHS Act).
This means that decision-makers need to collect appropriate information before making decisions. If the commissioner does not have the information, it needs then it should seek out appropriate advice. In many cases it will not be necessary to do this as all the necessary information is to hand.
The duty is most relevant to strategic decisions taken at directorate level within NHS
England, where decision-makers will need to document how they obtain advice from those with professional expertise (some of whom may be employees or secondees).
2.9 The duty to exercise functions effectively
The commissioner has a duty to exercise its functions effectively, efficiently and economically (in respect of NHS England, see section 13D of the NHS Act; and, in respect of ICBs, see section 14Z33 of the NHS Act).
This is a statutory reformulation of a duty that has been contained for many years in Managing Public Money and its predecessors. If the commissioner has complied with the other duties in this guidance – in particular, the duty to act reasonably – it is highly unlikely that it will breach this duty.
2.10 The duty not to prefer one type of provider
NHS England must not try and vary the proportion of services delivered by providers according to whether the provider is in the public or private sector, or some other aspect of their status (section 13P of the NHS Act). ICBs must also act in accordance with this duty when they are commissioning under delegated authority from NHS England.
This means that the commissioner must focus on the services delivered by an organisation and its sustainability. It should not make choices about contractors based solely on their status as, for example, company, partnership, public sector, private sector, charity or not for profit organisation.
Example
In partnership with local authority social services departments, the commissioner wishes to commission new in-reach support to support people living in care homes. It carries out a patient involvement exercise. Much of the feedback expresses a preference for the services to be delivered by a charity rather than a for profit organisation. However, the feedback does not give any reason for this. The feedback is a relevant consideration but in order to comply with its duty not to discriminate the commissioner should not prefer non- profit organisations, simply because they are non-profit.
2.11 Managing Conflict of Interest
NHS England must ensure it has appropriate processes in place to manage Conflict of Interest (C of I).
Conflicts of interest arise when an individual or organisation can exploit a professional or official capacity, including acquiring or using information or being involved in processes connected to contractual management of GDS services, for personal or business benefit. The existence of a conflict of interest does not, indicate that a person or organisation has acted in an unprofessional manner or breached any regulations. In some situations, conflicts of interest are unavoidable.
Conflicts of Interest are usually categorised in three ways:
- Actual – exists where financial or other personal or professional considerations compromise an individual’s objectivity, professional judgment, professional integrity, and/or ability to perform their responsibilities.
- Potential – exists in situations where an individual, a member of the individual’s family, or a close personal relation has financial interests, personal relationships, or professional associations with an outside individual or organisation, such that their activities within clinical advice could appear to be biased by that interest or relationship.
- Perceived – conflict of interest is described as this also, even if that individual has agreed not to act on those outside interests, as it could be viewed as a conflict by an interested or impartial party.
Examples of conflicts of interest that are relevant in healthcare include (N.B. this list is not exhaustive):
- Being a potential provider of services.
- Partnership (such as in a general practice) or employment in a professional partnership, such as a limited liability partnership.
- Directorships, including non-executive directorships held in private companies or PLCs.
- Ownership or part-ownership of private companies, businesses, or consultancies likely or possibly seeking to do business with the NHS or its Contractors.
- Shareholding in organisations likely or possibly seeking to do business with the NHS or its Contractors.
- A clinician making onward referrals to other establishments (which may be linked to an individual or business).
- Personal interest or that of a family member, close friend, or other acquaintance, in any of the above.
Part B – General contract management
3. Which dental contract when?
3.1 Introduction
There are three contract types that can be used when commissioning primary dental services: General Dental Services Contract (GDS), Personal Dental Services Agreement (PDS) both introduced in 2006 and a Personal Dental Services Plus Agreement (PDS+) developed in 2009 for procurements under the Dental Access Programme.
Dental services that can be commissioned under the GDS contract and PDS agreement includes:
- Mandatory services (General dental treatment);
- Additional services (Advanced mandatory services, Sedation services, Domiciliary services, Dental Public Health Services, Orthodontic services, Referral services);
- Further services which are not covered by Mandatory services or Additional services.
Examples of Further services includes level 2 Intermediate Minor Oral Surgery and level 2 Restorative services. Level 2 services can be provided within a primary care contract however they require a clinician with enhanced skills and experience due to the complexity of the procedure and or the patient.
Eligibility to hold a GDS contract is set out in the NHS Act 2006, Part 5 – Dental services, clause 102.
The NHS Act 2006 also sets out the right to hold a PDS agreement, in Part 5 Dental services, clause 108.
This chapter sets out the detail of who can hold a dental contract based on the rights set out in the Act.
Suitability to hold a GDS contract and PDS agreement is set out in the GDS and PDS Regulations 4 and 5.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 3.1: Persons eligible to enter into a GDS contract
- Annex 3.2: Persons eligible to enter into a PDS agreement
3.2 Comparison of dental contract type
|
Comparison of dental contracts |
GDS Contract (General Dental Services |
PDS Agreement (Personal Dental Services) |
PDS+ (Personal Dental Services |
|
Who can hold a contract? |
a) At least one partner is a dentist, and b) Any other partner is either NHS employee; a PDS/PMS employee (UK); a health care professional working in the NHS; or a PMS, GMS, PDS, or GDS provider (UK);
Please refer to Annex 3.1 for more detail |
Please refer to Annex 3.2 for more detail |
Same as PDS |
|
Where two or more individuals are practicing in partnership, is the contract treated as being made with the partnership? |
Yes |
No |
No |
|
Is the contract time limited? |
No Except in certain circumstances when a temporary GDS contract can be used (see Urgent Contracts below) |
Yes However, this does not mean an end date needs to be specified. Note that a PDS Contractor providing mandatory services may apply for a GDS contract any time prior to the end of the PDS agreement. See section 21 of the Personal Dental Services Agreements) Regulations. |
Yes As long as mandatory services are provided. Note that a right to a GDS contract also exists for PDS+ Contractors. See section 21 of the Personal Dental Services Agreements) Regulations. |
Can the commissioner terminate at will? |
No |
No |
No |
|
Must the Contractor provide mandatory services? |
Yes |
No |
No |
|
Can the contract contain KPIs? |
Yes |
Yes |
Yes |
|
Payment arrangements |
GDS SFE |
PDS SFE |
PDS SFE, Access and performance payments |
|
Model contract available |
Yes |
Yes |
Yes |
3.3 Temporary contracts
Circumstances may arise that require the commissioner to put in place a temporary contract. Such circumstances may include:
- the death of a Contractor
- the bankruptcy or insolvency of a Contractor
- termination of an existing contract due to patient safety
- termination of an existing contract due to the Contractor giving 3 months’ notice, when there is a need to re-procure the services
Before a decision to issue a temporary contract is made, Commissioners should undertake an options appraisal to confirm that a new contract is needed in their area, including whether activity should be redistributed.
The commissioner should comply with any relevant procurement guidance and organisational standing orders and standing financial instructions (SFIs).
Due to the short timeframes involved within points 1 – 3 of the above scenario, as part of the procurement process the commissioner may consider an application for a Single Tender Action which must be submitted and approved prior to the award of any temporary contracts.
Where continuity of services to patients is required, the short timescales involved may not allow the commissioner to undertake a managed closedown and transfer to a new provider. Please refer to Chapter 15 – ‘Practice Closedowns’ for further information. The commissioner may therefore look to award a contract to a specific party that is able to provide the services to patients at short notice.
Prior to awarding a contract in this scenario, the commissioner should consider a number of factors which are set out below.
3.3.1 Procurement
A direct award of a contract, without considering whether a competitive process is required to determine the new Contractor, risks being a breach of procurement law, in which case the commissioner could be challenged.
The following factors will be relevant in determining the extent of the risk:
- value of the new contract and whether it is best value for money
- duration of the new contract
- identity of the new Contractor and whether it can be argued that the new Contractor is the only provider capable of providing the services
- number of potential new Contractors
- cross-border interest of the new contract
- extent to which the need to procure a new contract was foreseeable
Where the commissioner determines that a contract for the immediate provision of services is required but time does not allow full consideration of the above factors (or for a competitive procurement process if required), the procurement risks can be mitigated by entering into a temporary contract as detailed above which provides time for the proper action to be arranged and followed. In addition, a commissioner may consider, in line with July 2022 policy announcements, the flexibility to allow, where resources are available, relevant contracts to deliver and be paid for up to 110% of contracted activity.
Having awarded a contract, the commissioner must maintain a record of how, in awarding the contract, it complied with its duties in relation to effectiveness, efficiency, improvement in the quality of the services and promoting integration.
3.3.2 Premises
The previous Contractor may own or lease the premises which, as a result, may not be available for the provision of the services under a new contract. The availability of the premises must be ascertained before entering into a temporary contract.
3.3.3 Public Involvement
One of the general duties of NHS England is to ensure there is public involvement where a decision leads to an impact on the provision of primary care services. If under a new contract, services are provided from a different location, this will be an impact on the services which may trigger the need to undertake a public involvement exercise.
Where there is no time for undertaking an exercise prior to entering into the contract, the commissioner should ensure that, as soon as possible after the contract is entered into, it arranges for such an exercise to be undertaken prior to the commissioner making any decisions about the long-term provision of services.
3.3.4 Commissioner Standing Orders (SOs) and Standing Financial Instructions (SFIs)
The commissioner may have organisational standing orders and standing financial instructions that require contracts to be procured in certain ways, e.g. securing three quotes for contracts up to a certain financial value. Where time does not allow the rules to be followed, there may be an emergency process that must be followed.
3.3.5 Other factors
Further factors may be relevant depending on the circumstances of the matter.
Please refer to Chapter 15 ‘Practice Closedowns’ for a list of all factors that may be relevant.
Commissioners should also consider that if a practice has closed because of concerns in relation to patient safety, the incoming provider may need to be commissioned to undertake a review of systems and processes. This should include but is not limited to, undertaking audits to provide assurance around patient safety. This recognises the additional work that Commissioners may need to reflect in the contract to provide assurance regarding patient safety and public confidence.
3.3.6 Which contract form?
GDS contracts are often considered unsuitable for a temporary solution as they are not time limited. However, a GDS contract can be used where the commissioner has terminated a contract of another provider of primary dental services, and because of that termination, it wishes to enter into a temporary contract for a period specified in the contract for the provision of services.
A time limited PDS agreement may not be attractive in this scenario as the PDS Contractor, if providing mandatory services, can request a non-time limited GDS contract at any time provided the Contractor gives at least three months’ notice of such request.
The commissioner should therefore consider what services and duration is required and whether there are any restrictions on the proposed Contractor entering into different contract types to meet local diverse health needs.
In addition, a commissioner may consider, in line with July 2022 policy announcements, the flexibility to allow where resources are available, relevant contracts to deliver and be paid for, up to 110% of contracted activity.
3.4 National clinical and legislative requirements
Contractors are expected to comply with any current and temporary operating standards that are introduced from time to time as required to meet the needs of the service.
4. Contract variations
4.1 Introduction
This policy describes the process for making contract variations, whether for all Contractors due to legislation changes or for individual contracts by mutual agreement.
As decisions made in relation to the contract/agreement can be disputed, it is essential that the commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 4.1: Template variation notice for legislation/regulatory change – GDS contract
- Annex 4.2: Template variation notice for legislation/regulatory change – PDS agreement
- Annex 4.3: General GDS contract or PDS agreement variation
- Annex 4.4: Notification of sub-contracting arrangements
- Annex 4.5: Request for information relating to change from individual to partnership – GDS contract
- Annex 4.6: Acknowledgement of information relating to change from individual to partnership – GDS contract
- Annex 4.7: Template variation relating to change from individual to partnership – GDS contract
- Annex 4.8: Request for information relating to change from individual to more than one individual – PDS agreement
- Annex 4.9: Acknowledgement of information relating to change from individual to more than one individual – PDS agreement
- Annex 4.10: Template variation relating to change from individual to partnership – PDS agreement
- Annex 4.11: Request for information relating to change from partnership to individual or remove a partner from a partnership – GDS contract
- Annex 4.12: Acknowledgement of information relating to change from partnership to individual – GDS contract
- Annex 4.13: Template variation relating to change from partnership to individual – GDS contract
- Annex 4.14: Request for information relating to change from more than one individual to an individual – PDS agreement
- Annex 4.15: Acknowledgement of information relating to more than one individual to an individual – PDS agreement
- Annex 4.16: Template variation relating to change from partnership to individual – PDS agreement
- Annex 4.17: Letter for single-handed practitioners requesting 24-hour retirement
- Annex 4.18: Contract variation for 24-hour retirement/partnership changes
4.2 Types of Contract Variation
Variations to contracts fall broadly within four categories:
- changes due to legislation or regulatory change;
- changes to the contracting party;
- changes to services; or
- changes to the payment arrangements.
Various contract variation templates have been provided within the appendices document which accompanies this policy book. If there is not a template available for the circumstances required, please use, and adapt the generic contract variation available in Annex 4.3.
All contract variations should include a paragraph explaining the change, the date of commencement and the relevant clause changes. The notice should be signed by all parties to the contract. Commissioners should ensure they follow the latest guidance on the use of electronic signatures.
Where a GDS contract or PDS agreement is varied and there is a change in the range of services provided, the Contractor must display written details of that change in a prominent position in a part of the premises to which patients have access. For example, if a Contractor stopped delivering sedation services at the practice.
The commissioner must inform those patients of the steps they can take to obtain elsewhere the services in question or seek treatment for the provision of mandatory services (or their equivalent).
Both Commissioners and Contractors are reminded that the over-arching aims during any contract variation process are to:
- ensure contracts reflect the reality of provision in accordance the GDS / PDS regulations
- safeguard continuity and quality of patient care
- minimise bureaucracy for both contractor and commissioner whilst ensuring that contracts and variations are up-to-date and properly recorded.
4.3 Legislation/regulatory changes
Usually both parties to a primary dental contract must agree a variation in order for it to take effect. The commissioner may, however, vary the contract without the Contractor’s consent where it is reasonably satisfied that it is necessary to do so to comply with the NHS Act, any regulatory changes pursuant to the NHS Act or any direction given by the Secretary of State pursuant to the NHS Act. This right is contained within all GDS contracts and PDS agreements.
The commissioner must notify the contractor in writing of the wording of the variation and the date it will take effect. Where it is reasonably practicable to do so, the date the variation will take effect must not be less than 14 days after the notice is served.
There is no need for the commissioner to seek agreement or require a signature of acceptance for this type of variation, as there is no right of refusal or negotiation.
A regulatory amendment to the existing GDS and PDS Regulations is issued under statutory instrument. Commissioners should ensure arrangements are in place to take the appropriate action as quickly as possible after the issue of an amendment.
Where the GDS Regulations are amended, there may be a centrally issued GDS variation to the Standard GDS Contract and a supporting notice both of which should be used to inform the Contractors of the change. This is not possible for PDS agreements as these are locally defined, which vary significantly across the country. Commissioners will therefore need to action this locally.
The commissioner must notify contractors of the variation and its effective date. A template variation letter is provided in Annex 4.1 for GDS contracts and Annex 4.2 for PDS agreements. A general template variation notice is provided at Annex 4.3 which can be used for this purpose.
For GDS Contractors, the notification should include the GDS variation and the relevant pages of the amended contract document for completeness. For PDS Contractors, the commissioner will be required to ensure the regulatory amendments become a contractual amendment, citing the correct clause numbers affected within the individually held contracts and including the relevant pages of the document for completeness.
All electronically held contracts should be updated with the variations at this stage to ensure that the centrally held documents remain up to date with current legislation.
Commissioners should retain a copy of the notice on file for completeness. Each contract file should contain a variation log and Commissioners should ensure that this is updated accordingly.
4.4 Changes to the contracting party
Changes to the contracting party may be due to:
- partnership changes;
- company changes;
- retirement (including 24-hour retirement);
- novation’s, mergers, and splits; and
- death of a Contractor.
There are specific processes to follow on the death of a Contractor. Please refer to Chapter 12 ‘Death of a Contractor’ for further information.
The GDS Regulations and PDS Regulations contain provisions relating to the remaining scenarios listed above which are considered in more detail below.
4.5 Sub-contracting
The GDS and PDS regulations allow for the provision of clinical matters to be subcontracted to another provider. Sub-contracting is defined as the process of assigning or outsourcing, part of the obligations under a contract to another party who is then known as a sub-contractor.
Sub-contracting within dental contracts allows the clinical care to be provided by another party, however in these circumstances the contractual relationship remains between the commissioner (the NHS) and the contractor. This is not sub-contracted.
Standard GDS contracts and PDS agreements detail sub-contracting as shown below:
4.5.1 Sub-contracting of clinical matters
The Contractor shall not sub-contract any of its rights or duties under the GDS contract or PDS agreement to any person in relation to clinical matters unless:
- It has taken reasonable steps to satisfy itself that:
- it is reasonable in all the circumstances, and
- that the person is qualified and competent to provide the service; and
- It is satisfied in accordance with clauses 251to 254 that the sub-Contractor holds adequate insurance.
- It is satisfied that there is an expectation that contracted activity / access levels are maintained
- It is satisfied that the relevant superannuation rules have been applied to the sub-contracting party. Further guidance on this can be found on the NHSBSA website (published August 2021).
Where the Contractor sub-contracts any of its rights or duties under the GDS contract or PDS agreement in relation to clinical matters, it shall:
- inform the commissioner of the sub-contract as soon as is reasonably practicable; and
- provide the commissioner with such information in relation to the sub-contract as it reasonably requests.
Where the Contractor sub-contracts clinical services in accordance with clause 198, the parties to the contract shall be deemed to have agreed a variation to the agreement which has the effect of adding to the list of the Contractor’s premises any premises which are to be used by the sub-contractor for the purpose of the sub-contract and clause 287 shall not apply.
It is the responsibility of the Contractor to ensure that superannuation returns are correct.
A contract with a sub-contractor must prohibit the sub-contractor from sub-contracting the clinical services it has agreed with the Contractor to provide.
Some local contracts/agreements include additional requirements/restrictions, so Contractors should confirm the terms of their contract/agreement before proceeding to notify of sub-contracting.
A Contractor does not have to subcontract the whole of the contract; therefore, a notification may be received from a Contractor wishing to subcontract part of their contract, for example 30% of their UDAs, or sub-contract their additional services element but continue to provide mandatory services.
To provide the necessary assurance of appropriate sub-contracting arrangements the form at Annex 4.4 should be used by Contractors to notify the commissioner.
On receipt of the completed Annex 4.4 the commissioner should take a view on whether the sub-contracting arrangement proposed is reasonable in all circumstances. Where the commissioner feels that the proposed sub-contracting arrangements are reasonable in all circumstances then there is no requirement to vary the contract. In such circumstances the contract payment system will need to be updated to reflect any additional premises and performers involved in the delivery of the sub-contracting, as well as timescales, including start and end date.
If the commissioner feels that the proposed sub-contracting arrangements are not reasonable in all circumstances, then a dialogue should be opened with the contractor to reach a mutually acceptable arrangement. This may involve following the local dispute resolution process. See Chapter 13 ‘Managing Disputes’ for further information.
4.6 Partnership changes
Changes to the composition of a partnership will require variation to the contract and may require a variation to the standard registration conditions with the CQC.
Procurement law may be relevant as, in some circumstances, adding a new contracting party may give rise to procurement obligations. Commissioners should refer to relevant published guidance and should take appropriate advice at an early stage. Commissioners must also act in accordance with any procurement protocol issued by NHS England.
The Regulations place restrictions on the organisational structures that are eligible to enter into different types of primary dental contracts.
Please refer to Chapter 3 ‘Which Dental Contract When?’ for details on the eligibility criteria.
Contracts may be varied in several ways with relation to partnership matters, including the following which are looked at in more detail below:
- individual Contractors changing to more than one individual (which may be a partnership requiring a different process depending on whether it is a GDS contract or PDS agreement);
- changes to the parties of contracts with more than one individual (which may be from a partnership to an individual Contractor or changes to the composition of partnerships); and
- disputes between partners or members.
4.6.1 Individual to partnership – GDS contracts
If a GDS Contractor is currently an individual dental practitioner who wishes to enter into partnership with one or more individuals under that contract, the contractor is required to notify the commissioner in writing and provide the following information:
- the name of the person or persons with whom the contractor proposes to practice in partnership;
- confirmation that the person or persons is either:
- a dental practitioner; or
- a person who satisfies the conditions specified in section 102(2)(b) of the NHS Act;
- confirmation that the person or persons satisfies the conditions imposed by regulation 4 of the GDS regulations;
- whether or not the partnership is to be a limited partnership and if so, who is a limited partner and who is a general partner; and
- the date on which the contractor wishes to change its status (which shall not be less than 28 days from the date on which the notice was served on the commissioner).
Commencement of the new contract should be made conditional on the new Contractor being CQC registered. The CQC will issue a sales and transfer position statement document, but this is no guarantee of registration. A practice cannot commence seeing patients until they have received their registration certificate with the regulated activities (surgical procedures, treatment of disease, disorder, and injury) included. Further guidance on CQC registration is available on their website.
The notice must be signed by the individual Contractor and by the person or persons with whom the individual Contractor is proposing to practise in partnership. Where a Contractor contacts the commissioner about such a change, the commissioner should send Annex 4.5.
The commissioner must ensure the accuracy of the information provided. This may be achieved, for example, by checking the registration status of the proposed partner(s) and that the proposed partner(s) meet the eligibility criteria for holding a GDS contract.
Commissioners shall confirm in writing that the contract will continue with the partnership and issue a variation notice (two copies) accordingly to amend the relevant sections of the contract. All partners should sign the contract variation. The commissioner must specify in the notice the date on which the contract will continue as a partnership. Where reasonably practicable this should be the date requested by the contract holder in their initial notice, or the nearest date to it. However, it can only be actioned on the date requested by the Contractor where all relevant checks have been concluded and CQC registration is in place. A template acknowledgement letter is provided in Annex 4.6.
A variation notice must include the wording of the proposed variation and the date on which the variation will take effect. A template variation notice is included at Annex 4.7. The Contractor would then be required to return both signed copies of the variation notice, which the commissioner will sign once received. Once received, the commissioner should sign both copies and return one version of the signed to the Contractor. The commissioner should ensure that the electronically held contract documentation is amended accordingly.
If the Contractor does not return a signed copy of the variation notice, then the variation does not take effect and the contract continues as an individual.
If a new partner(s) is / are not accepted as eligible the commissioner should advise the contractor in writing of the reason(s) they believe the proposed partner(s) to be ineligible and confirm that the contract status will remain an individual contractor until the matter can be resolved, or a further notice is provided by the contractor proposing an alternative eligible partner. If the contractor wishes to dispute the decision, they can do so by following the dispute process set out in Chapter 13.
4.6.2 Individual to more than one individual – PDS agreement
The PDS Regulations allow PDS agreements to be agreed with limited liability partnerships but do not allow PDS agreements to be treated as made with general or limited partnerships.
Where individuals are practising in general partnership (not a limited liability partnership), the PDS agreement will be entered into with each individual. The individual signatories to a PDS agreement collectively form the contractor. The term individual in this circumstance covers all parties that are eligible to hold a PDS agreement for example an NHS Trust. Please refer to Chapter 3 ‘Which Dental Contract When?’ for further information.
The PDS Regulations do not require a PDS agreement to define a specific process for any variation to the signatories. The commissioner must, therefore, review the relevant PDS agreement to determine whether any provisions have been added relating to this and prior to following any process for variation.
If the Contractor is currently an individual dental practitioner and they wish to have one or more individuals join them under that agreement, then they must seek the Commissioner’s consent in writing for any such variation to the contract.
Where a Contractor contacts the commissioner about such a change, the commissioner should send Annex 4.8. The commissioner must have consideration of any procurement implications, along with other influencing factors, when considering such an application.
The commissioner must ensure the proposed individual(s) meet the eligibility criteria for holding a PDS agreement. Please refer to Chapter 3 ‘Which Dental Contract When?’ for further information.
Commencement of the new PDS agreement should be made conditional on the new Contractor being CQC registered. The CQC will issue a sales and transfer position statement document, but this is no guarantee of registration. A practice cannot commence seeing patients until they have received their registration certificate with the regulated activities included. The effective date of the contract variation also needs to align with the CQC registration date and cannot precede this.
The commissioner should confirm its decision on the variation in writing to the Contractor detailing the reasons for the decision and details of any information that they have relied upon in the process. A template acknowledgement letter is provided in Annex 4.9.
If the decision is to consent to the variation, then the commissioner shall issue a variation notice (two copies) accordingly to amend the relevant sections of the contract. A variation notice should include the wording of the proposed variation and the date upon which the variation will take effect. A template variation notice is included at Annex 4.10. The contractor would then be required to return both signed copies of the variation notice. Once received, the commissioner should sign both copies and return one version of the signed to the contractor. The commissioner should ensure that the electronically held contract documentation is amended accordingly.
If the contractor does not return a signed copy of the variation notice, then the variation does not take effect and the contract continues as an individual.
If the new signatory is not accepted as eligible the commissioner should advise the contractor in writing of the reason(s) they believe the proposed signatory(ies) to be ineligible and confirm that the contract status will remain as it was, until the matter can be resolved, or a further notice is provided by the contractor proposing an alternative eligible signatory. If the contractor wishes to dispute the decision, they can do so by following the dispute process set out in Chapter 13.
4.6.3 Changes to contracts with more than one individual – GDS contracts
There are two ways that a partnership can change:
- if it is dissolved or terminated; or
- the composition changes.
Both scenarios are explained below.
4.6.4 Partnership to individual
There may be a time in the life of a partnership where the partnership is terminated or dissolved. This may be based on an agreement between partners but may also come about due to a dispute between the partners. Where a partnership is dissolved or terminated, and the contractor consists of two or more individuals practising in partnership, the contract will terminate. The contract may, however, continue with one of the former partners if the following conditions apply:
- the former partner must be nominated by the contractor and all parties to the contract; and
- the former partner must be a dental practitioner
The nomination of the former partner by the Contractor must:
- be in writing and signed by all the persons who are practising in partnership. Where a Contractor contacts the commissioner about such a change, the commissioner should send Annex 11
- specify the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner
- be provided to the commissioner at least 28 days in advance of the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner
- specify the name of the dental practitioner with whom the contract will continue, which must be one of the partners.
Where the commissioner receives the information, it must acknowledge receipt of the notice in writing before the date specified in the nomination as the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner. A template notice is provided in Annex 4.12. A variation notice will need to be included with this letter. The commissioner must notify the Contractor in writing of the wording of the proposed variation and the date upon which that variation is to take effect.
Where the commissioner agrees the nomination, the commissioner may vary the contract but only to the extent that it is satisfied it is necessary to reflect the change in status of the Contractor from a partnership to an individual dental practitioner. A template variation notice is included at Annex 4.13. The notice should be signed by all parties to the contract, including the partner(s) who are leaving the contract.
The commissioner should be satisfied that the arrangements in place for continuity of service provision are robust.
In circumstances where the commissioner is not satisfied that the nominated partner is eligible to hold the contract as an individual, they should enter into dialogue with all of the partners, to explore potential solutions.
These might include the partners nominating an alternative partner to continue with the contract, in which circumstances a new notice should be issued to the commissioner to include these details and propose a new date on which the changes will occur.
4.6.5 Partnership – composition change
Where the Contractor consists of two or more individuals practising in partnership and the composition of the partnership changes, either by a partner leaving (but without the partnership terminating) or a new partner joining, the contract will need to be amended to recognise the new partnership composition.
The following process should be followed in the above scenario:
- The partnership issues notice to NHS England setting out:
- the date that the new partner(s)intend to join or have joined the partnership;
- confirms that the new partner(s) are a dental practitioner, or that they satisfy the conditions specified in Section 102 of the NHS Act;
- confirms that the new partner(s) meet the conditions imposed by regulation 4 of the GDS Regulations; and state whether the new partner(s) are general or a limited partner(s);
- confirms that the relevant notification has been made to CQC or is in the process of being made. Further guidance on the notification required to CQC about partnership changes can be found on the CQC website.
- The commissioner would then issue a variation notice in writing (two copies) to be signed by all parties to the contract (e.g. signed by all partners) ensuring that all partners agree with the proposed partnership change.
If the Contractor does not return a signed copy of the variation notice, then the variation does not take effect and the contract continues as it is.
The commissioner should be aware that where the Contractor is two or more persons practising in partnership, the commissioner may terminate the contract where one or more persons have left the practice during the existence of the contract. This right of termination only arises where the commissioner, in its reasonable opinion, considers that the change of membership of the partnership is likely to have a serious adverse impact on the ability of the contractor or the commissioner to perform their obligation under the contract (clause 339).
If the commissioner intends to rely on this right of termination, please refer to Chapter 11 ‘Contract Terminations and Sanctions’ for further information on this right and on termination generally.
4.6.6 Changes to contracts with more than one individual – PDS agreements
The PDS Regulations do not require a PDS agreement to define a specific process for any variation to the signatories. The commissioner must, therefore, review the relevant PDS agreement to determine whether any provisions have been added relating to this and prior to following any process for variation.
If the Contractor is currently two or more individuals and wish to remove a signatory to the agreement so that it reverts to either a single signatory or fewer signatories, then they must seek the Commissioner’s consent in writing for any such variation to the agreement. Where a contractor contacts the commissioner about such a change, the commissioner should send Annex 4.14. The commissioner must consider any procurement implications, along with other influencing factors, when considering such an application.
The commissioner must ensure that the proposed individual meet the eligibility criteria for holding a PDS agreement please refer to Chapter 3 ‘Which Dental Contract When?’ for further information.
Commencement of the new agreement should be made conditional on the new Contractor being CQC registered. The CQC will issue a sales and transfer position statement document, but this is no guarantee of registration. A practice cannot commence seeing patients until they have received their registration certificate with the regulated activities included.
The commissioner should confirm its decision on the variation in writing to the contractor detailing the reasons for the decision and details of any information that they have relied upon in the process. A template letter is provided in Annex 4.15.
If the decision is to consent to the variation, then the commissioner must issue a variation notice (two copies) accordingly to amend the relevant sections of the agreement. A variation notice should include the wording of the proposed variation and the date upon which the variation will take effect. The Contractor would then be required to return both signed copies of the variation notice. Once received, the commissioner should sign both copies and return one version of the signed to the Contractor. The commissioner should ensure that the electronically held contract documentation is amended accordingly.
If the Contractor does not return a signed copy of the variation notice, then no amendment to the agreement can take place.
If the remaining individual to the agreement is not accepted as eligible the commissioner should advise the Contractor in writing of the reasons, they believe the individual is ineligible and confirm that the agreement status will remain as it was until the matter can be resolved or a further notice is provided by the Contractor proposing an alternative eligible individual.
The principles outlined will also apply where the contractor consists of two or more individuals and the composition of the Contractor changes, either by an individual wishing to leave the agreement or a new individual joining the agreement. The agreement will need to be varied to recognise the new contractor composition. A template variation notice is included at Annex 4.16.
The commissioner should ensure that it is satisfied that the contractor will remain eligible to hold the agreement after the variation. For the variation to have effect, it must be in writing and signed by all existing (and new) individuals to the agreement.
The commissioner should also be satisfied that the arrangements for continuity of service provision to the local population covered within the contract are robust and may wish to seek written assurances of the post- variation Contractor’s ability and capacity to fulfil the obligations of the agreement and their proposals for the future of the service.
GDS contracts are required to contain a right of termination where one or more partners has left the practice during the existence of the contract. PDS agreements are not required to contain such a right of termination. The commissioner should therefore review the relevant PDS agreement to determine whether any such provision has been included.
4.6.7 Partnership splits/members dispute – GDS and PDS
Where the Contractor to a GDS contract is a partnership and the partnership dissolves due to an internal partnership dispute, the contract will terminate unless the parties agree for the contract to continue with one partner. The commissioner may have little time to make arrangements to ensure service continuity.
It is, therefore, desirable that the partners of a GDS contract can resolve disputes internally where possible, with the support of the LDC and/or mediation services.
If the partnership holding a GDS contract does not dissolve or terminate but the partnership no longer wishes to hold a GDS contract, then the contractor will need to terminate on notice, which must not be less than three months unless agreed by the commissioner. Failure to give three months’ notice of termination is a breach of contract and the appropriate action may be taken in line with the policy on contract breaches. See Chapter 10 – ‘Contract breaches’ for further information.
Under PDS agreements, subject to the terms of the individual agreements, partnership matters (including dissolution or termination of the partnership) do not affect the continuation of the agreement. This is because where the agreement is with two or more individuals that are practising in partnership, the agreement is not entered into with the partnership but instead with the individuals (who collectively make up the contractor).
If a PDS agreement is held by more than one signatory and those signatories separately operate as a partnership, following termination of that partnership, or if any signatory no longer wishes to be a party to the PDS agreement, the contractor will need to give notice to terminate the agreement, such notice being a minimum of three months unless agreed with the commissioner. Please refer to Chapter 11 ‘Contract Terminations and Sanctions’ for more information.
Where partnerships or membership are formalised through a partnership agreement, it is helpful if the parties can rely on the detail of these agreements to support the early resolution of internal disputes and to ensure that such agreements are reviewed and maintained to be current with associated legislation.
Unfortunately, many partnership organisations do not have agreements in place or have insufficient or outdated documents which can often lead to very protracted and acrimonious disputes between the partners.
The commissioner should not get involved in endeavouring to resolve the dispute between the partners, instead insisting that the parties notify the commissioner of their final decision when it is reached.
It is likely that the commissioner will have numerous contacts from different partners and their staff regarding the dispute, but the commissioner should try to maintain a detached position in this respect. Any accusations of inappropriate behaviour or concerns should be considered; however, this should not be used to resolve the dispute.
Throughout the dispute the Commissioners should maintain open dialogue with the LDC and implement contract performance management protocols, when necessary.
4.7 Retirement of a contractor – single handed
There is no specific reference to retirement in the GDS and PDS Regulations. The commissioner should deal with a request to retire as a request to terminate the contract by the Contractor on notice.
The contractor must provide the commissioner with a written notification of the intended retirement date which will be the termination date of the contract. This notice period must not be less than three months. If the termination date is not the last calendar day of a month, the contract shall instead terminate on the last calendar day of the month in which the termination date falls. For example, if the termination date is the 16 April, then the contract will terminate on the 30 April.
In exceptional circumstances, such as ill health, the commissioner may wish to waive its right to the full notice period, but it remains its right alone to do so. Consideration should be given, amongst other matters, to the effect that holding a contractor who is unwell to the full notice term may have on the contractor, the practice’s patients, and colleagues.
In either case the commissioner should confirm receipt and acceptance of the retirement/termination notice in writing, the date on which the contract will terminate and any consequences and actions that the contractor must take because of the notice.
Although not required by the GDS Regulations, the Standard GDS Contract clearly sets out the arrangements that must be made on termination of a contract, which include (but are not limited to) the Contractor having to:
- cease performing any work or carrying out any obligations under the contract
- co-operate with the commissioner to enable any outstanding matters under the contract to be dealt with or concluded satisfactorily
- co-operate with the commissioner to enable the Contractor’s patients to be transferred to one or more other Contractors or providers of mandatory services (or their equivalent)
- deliver up to the commissioner all property belonging to NHS including all documents, forms, computer hardware and software, drugs, appliances, or dental equipment which may be in the Contractor’s possession or control
The commissioner shall have in place arrangements for collecting any property owned by the NHS on or immediately after the termination date, which should be included on a log of collection, and against any the commissioner held asset list, and where possible the Contractor should be asked to sign to confirm the property that has been removed, accepting that it is owned by the NHS.
On termination of the contract, the commissioner shall perform a reconciliation of the payments made by the commissioner to the contractor and the value of the work undertaken by the contractor under the contract. The commissioner must then serve the contractor with written details of the reconciliation as soon as reasonably practicable, and in any event no later than 28 days after the termination of the contract.
Each party shall pay the other any monies due within three months of the date on which the commissioner served the contractor with written details of the reconciliation, or the conclusion of any NHS dispute resolution procedure, or court action as appropriate.
The key elements for consideration leading up to a termination remain the same in respect of patients, property and transfer of records and confidential information.
For a list of considerations relating to termination, please refer to Chapter 11 ‘Contract Terminations and Sanctions’.
4.8 Retirement of a contractor – two or more partners/individuals
Where a partner wishes to retire from a GDS partnership, as constituted from time to time, the Contractor will need to notify the commissioner that it wishes to vary the contract. The commissioner should follow the process as detailed under the sub-heading changes to contracts with more than one individual – GDS contracts.
Where an individual wishes to retire from a PDS agreement, where that agreement is also held by one or more other individuals, the Contractor will need to notify the commissioner that it wishes to vary the agreement. The commissioner should follow the process as detailed under the sub-heading changes to contracts with more than one individual – PDS agreements.
The commissioner should always keep in mind the possible implications on procurement and competition when applying the guidance in this policy.
Any changes to the partners within a contract may require a new registration with CQC. The commissioner must ensure that the contractor has received CQC registration or where this has not yet been achieved the sale and transfer position statement from the CQC for the new partnership arrangements.
4.9 Twenty-four-hour retirement
When a contractor wishes to take their pension there will be different requirements based on the pension scheme, they are in. Where a contractor is a member of the 1995, 2008, or 2015 pension schemes to access their NHS pension they must retire from all NHS contracts that they hold and not return for 24 hours. Where they hold a contract as an individual this will mean the termination of their contract. However, many contractors wish to take their retirement without losing their contract.
Where the contract is an individual contract holder, they often do not want to terminate their contract and they look to avoid this by becoming a partnership. However, they do not wish this to be a long-term arrangement, and so look to undertake a process called 24-hour retirement.
Where a member of the 1995 Section membership of the NHS Pension Scheme takes their normal NHS age pension, voluntary early retirement pension, or deferred (including ill health deferred) pension they are no longer subject to the ‘16 hour a week rule’ in the first calendar month.
Members of the 1995, 2008 or 2015 schemes can also take ‘partial retirement’ which means they are not required to retire from all NHS contracts they hold but must reduce their commitment to the NHS by at least 10%. This option is attractive to ‘single-handers’ as they do not have to give up their GDS contract or PDS agreement.
If the commissioner is approached by a Contractor wishing to take 24- hour retirement, it must not offer advice relating to pension arrangements. Contractors should be sign posted to NHS Pensions for professional advice.
Further information on pensions, can be found in the NHS Pensions Guide for NHS General Dental Practitioners.
Contractors should ideally provide three months’ notice of their retirement to both the commissioner and NHS Pensions. This is in line with the pension requirement and also the notice period for the termination of their contract.
Where a Contractor confirms that to take their pension they will need to retire from the contract, steps will need to be taken to ensure that the contractor is removed from the contract, either by:
- termination on notice in the case of a single-handed contractor; or
- termination or variation of the contracting party in the case of a partnership.
The commissioner may wish to suggest single-handed practitioners take independent legal advice, as 24-hour retirement using the method described above would necessitate the termination of the contract. Please refer to Annex 4.17 for a template letter to send to single-handed providers who are interested in 24-hour retirement.
The commissioner must make clear to the contractor that there is no guarantee that the commissioner would commission services from that individual following termination of their current contractual arrangement.
If the GDS contract is held by a partnership or a dental body corporate, or the PDS agreement held by more than one individual, it will not automatically be terminated when an individual named as a partner or director takes 24-hour retirement, as the contracting party (i.e. the remaining partner(s) individual(s) or dental body corporate) continues to be the provider of the contract during the period for which the individual is retired. However, the make-up of the directors would need to meet the 50/50 requirement of clinical to lay people. If no other directors are dental care professionals, they would need to consider taking on another dental care professional as a director for the contract to continue during the 24-hour retirement.
4.9.1 24-hour retirement process
The single-handed Contractor may wish to go into partnership to facilitate their 24-hour retirement and the continuation of their contract. A new partner would be subject to the necessary checks as detailed in the GDS Regulations. Individuals may request to form a partnership under a GDS contract at any time using clause 292. These changes would normally need to follow the usual time frames for variations, however where a 24-hour retirement is being requested this can be managed differently.
If there are no concerns about the provider entering into partnership, the Commissioner will request the provider submits a 292 notice (signed by both parties) stating the date the partnership will be formed and the 231 Notice (signed by both parties) which states the date that the contract will revert to an individual. It may be prudent for the Commissioner to ensure that the original provider is eligible to hold the contract at the same time as the new partner, as although they are an existing contract holder, once they are removed, the retiring provider would be subject to the same GDS/PDS performer checks.
On receipt of the above the Commissioner would issue the relevant contract variations, which can be prepared as a pack and issued for signature in advance of the retirement:
- Individual A to partnership A and B
- Partnership A and B to individual B
- Individual B to Partnership A and B
- Partnership A and B to Individual A
The contract variations should include the following clause:
“This variation is made to enable [name of individual] to apply for 24-hour retirement from the NHS contract, to satisfy the NHS pension scheme regulations. The registration of this partnership with the Care Quality Commission (CQC) is unlikely to be required if the partnership will not be delivering any regulated activities during the period for which the NHS contract is held by the partnership. The contract held by [partnership name] will revert to being held by [name of individual] on [date].”
Annex 4.18 provides a template for use in these circumstances.
The Commissioner may consider undertaking an options appraisal, to give due consideration to the procurement regulations including:
- “New award” is unlikely to be visible to the market
- the contract is not ostensibly due for renewal (and so the market will not be looking for the new opportunity to be available)
- the practice of 24-hour retirement has been accepted historically
- the duration and other terms and conditions of the GDS contract will not change from the original GDS contract and therefore there is no material change; and/or
- This options appraisal should include appropriate legal advice and be signed off via each team’s local governance process.
The Commissioner should seek legal advice for further information on procurement implications.
5. Bodies corporate – variations and incorporations
5.1 Introduction
GDS contracts and PDS agreements may be held by different types of bodies corporate. Please refer to Chapter 3 ‘Which Dental Contract When?’ for a summary of the types of bodies corporate.
There are various eligibility and suitability criteria that must be satisfied before any of these types of organisations can hold GDS contract or PDS agreements. For further information, please refer to Chapter 3 ‘Which dental contract when?’.
A change to or from an individual or partnership Contractor to or from these types of organisations is a complete change of the identity of the contracting party, regardless of whether the organisation is owned and/or run by the original Contractors. This will technically require termination of the existing contract and immediate replacement with a new contract on the same terms. This is a contract novation and is explained further below.
Where the novation involves a transfer of the contract from an individual or partnership to a corporate body, this is often referred to as “incorporation”. Where the novation involves a transfer of the contract to an individual or partnership from a corporate body, this is often referred to as “dis- incorporation”. Such changes will not technically be a variation to the original contract as the original contract will be replaced by the new contract.
As decisions made in relation to the contract / agreement can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 5.1: Acknowledgement of request to incorporate
- Annex 5.2: Dental incorporation application form5.3Assessment template for incorporation for Commissioner
- Annex 5.4: Acknowledgement of request to dis-incorporate
- Annex 5.5: Dental dis-incorporation application form
- Annex 5.6: Assessment template for dis-incorporation for Commissioner
- Annex 5.7: Refusal of request to [incorporate/become a company limited by shares
- Annex 5.8: Refusal of request to dis-incorporate
- Annex 5.9: Template agreement letter
- Annex 5.10: Novation Agreement
- Annex 5.11: NHS Dental Services Payment System
5.2 Contract novation and incorporation/dis-incorporation
Incorporation of a GDS agreement usually occurs where a Contractor that is an individual or a partnership wishes to transfer the agreement to a dental corporation or a limited liability partnership.
Incorporation of a PDS agreement usually occurs where a Contractor that is one or more individuals wishes to transfer the agreement to a dental corporation, a company limited by shares or a limited liability partnership.
Dis-incorporation is the same process in reverse.
Where one party to a contract (A) proposes to completely remove itself from the contract to be replaced by a separate party (B), this cannot be a variation to the contract. Instead, this is a transfer of the rights and obligations under the contract which is termed a contract novation.
A contract novation is not a variation. A novation agreement must be signed instead. This ends the contractual relationship between the Commissioner and old Contractor and creates a new contractual relationship between the Commissioner and new Contractor on the same terms. From a procurement perspective, the novation agreement counts as awarding a new contract. Where a new contract is awarded, although it may be a contract novation or may be on the same terms as the original contract, there may be procurement law implications.
Commissioners must also act in accordance with any procurement protocol issued by NHS England.
A contract novation is often requested where a person or company is selling its business and as part of the sale it is transferring its contracts and its customers to the buyer. The contracts are novated, and the buyer agrees to take over the seller’s responsibilities for performing the contracts and takes on any associated debts and obligations.
There is no express right for a Contractor to incorporate or dis-incorporate a contract. Contractors should be made aware that incorporation or dis-incorporation could potentially result in the Commissioner deciding to competitively tender the new contract in accordance with procurement law. The Contractor to the original contract may not be successful in winning the new contract.
5.2.1 Managing a request for incorporation or dis-incorporation
On receipt of a request from a Contractor to incorporate or dis-incorporate, the process below should be followed:
- The Commissioner should acknowledge the request and send the Contractor an assessment template. A letter and the assessment template for incorporation are provided in Annex 5.1 and 5.2 with a form for internal Commissioner use provided in Annex 5.3.
- A letter and assessment template for dis-incorporation are provided in Annexes 5.4 and 5.5 with a form for internal Commissioner use provided in Annex 5.6
- The Commissioner should make the Contractor aware of the potential implications of the incorporation or dis-incorporation.
- On receipt of the information, the Commissioner should review the information and decide whether to agree the request.
The Commissioner should first consider whether the proposed new Contractor is eligible to enter into the contract. If it is not eligible, the Commissioner must refuse the request. A template letter of refusal of a request to incorporate is provided in Annex 5.7 and in respect of dis-incorporation in Annex 5.8.
Commissioners should undertake an options appraisal to confirm that a new contract is needed in their area. This opportunity should be taken to evaluate whether activity needs to be re-distributed.
Additionally, Commissioners should seek additional benefits to ensure that services meet the needs of the local population.
Where the proposed Contractor is eligible, the Commissioner should consider a number of further matters listed below. In considering these matters, the Commissioner, is required to act reasonably and otherwise in accordance with public law principles:
- the Commissioner’s obligations under procurement law to determine whether there is a risk of challenge in agreeing the request or whether a competitive tender process should be carried out;
- the effect of the proposal on the statutory duties of NHS England, particularly the duty under Section 13K of the NHS Act (duty to promote innovation) and Section 13P (duty as respects variation in provision of health services) – for further information, please refer to chapter 4 (General duties of NHS England)
- the value of the contract
- the level of market interest
- the potential for innovation
- the need to protect services in the core contract
- continuity of patient care
- the extent to which the original Contractor(s) will be controlling and giving instructions to the proposed Contractor to comply with contractual obligations
- that extent of change to the terms of the existing and new contract (i.e. contract value or activity level)
- payments under the existing contract and value for money
- benefits to service users of the proposal
- amendments to the activity level in the contract, e.g. where there has been previous underperformance, the commissioned UDAs or UOAs may be reduced to a realistic and achievable level
- opening hours (including evening and weekend) and urgent access slots required
- whether the Commissioner requires that the existing Contractor guarantees the performance of the proposed Contractor – any such requirement must be proportionate to the risks associated with the novation and reasonable with a clear rationale for placing such a responsibility on the existing Contractor – legal advice should be sought
- whether the proposed Contractor is a company but is not registered with Companies House (the Contractor may take the view that this cannot be finalised until agreement in principle has been given by the Commissioner)
- whether any director of the company has been disqualified from another registered company (check Insolvency Website and Companies House Disqualified Directors); or received an unsatisfactory Disclosure and Barring Scheme
- the potential to review any restricted contracts; for example, the contract is restricted to child/exempt only and whether the restrictions should be removed
- whether the existing Contractor has outstanding NHS debts which may include repayment due to underperformance from previous years and whether novation is made conditional on repayment being made
- whether the existing Contractor has received a breach or Remedial Notice and whether novation is made conditional on the proposed Contractor taking on the consequences of the notices (e.g. action the remedial activity)
- whether the circumstances that led to the issue of a Breach Notice or a Remedial Notice has any relevance to the request for incorporation/disincorporation particularly where the Contractor has complied with any Remedial Notice issued; and/or
- whether the existing Contractor has outstanding issues regarding CQC inspection or practice inspection by the Commissioner and whether the novation should be made conditional on those issues being resolved.
Requests for incorporation or dis-incorporation should be agreed with or without conditions unless there are concerns as to whether a request would present a benefit to patients or create a significant risk of successful procurement law challenge.
5.2.2 Agreeing the request
Where the Commissioner agrees the request, the original contract will be novated. Novation in contract law is a mechanism whereby one-party transfers all of their obligations and benefits under a contract to a third party. The original contract is terminated, and a new contract is created.
Legal advice should be sought on whether a deed or a simple novation agreement should be used. The difference between a deed of novation and a novation agreement is that the former must be signed under seal. A novation agreement does not require the seal and can be signed by the appropriate person within the commissioning team. A template novation agreement is provided in Annex 5.10 along with a template letter agreeing to the change in Annex 5.9.
The Commissioner should ensure that the Contractor has adhered to points 1.1.1 and 1.1.2 in Annex 5.11 before any approval is given.
The novation agreement is a template and will need to be adapted to reflect the novation situation, for example:
- individual to company where individual is the only director/shareholder
- individual to company with individual and others as directors/shareholders
- individual to company with others as directors/shareholders
- company to company
As a contract novation is technically termination of the original contract and replacing it with a new contract, new contract documentation should be issued to the Contractor alongside the deed of novation/novation agreement.
If the Contractor does not return a signed copy of the contract document and deed of novation / novation agreement, then no changes can take place.
The Commissioner must make appropriate arrangements for the termination of the original contract including:
- carrying out a financial reconciliation
- managing any under performance in terms of financial recovery, service delivery or performance concerns and details of how these will be managed going forward
- any other requirements in the contract relating to termination
The Commissioner will need to agree a new contract with the new Contractor which may vary from the original contract in terms of services provided, numbers of UDAs and UOAs and any other changes agreed.
As the request is for incorporation, the new Contractor will be a body corporate therefore the novation agreement includes a change of control clause. Such a clause requires the Contractor to notify the Commissioner where there is a change in ownership or control of the Contractor. A standard change of control clause is included in the Novation Agreement provided in Annex 5.10. This clause means that the new Contractor cannot change the shareholders without the prior consent from the Commissioner. However, this consent should not be unreasonably withheld or delayed. This removes the limitation of how much of the ownership can change without permission and allows the Commissioner to understand who the ‘owner’ of the contract is.
Where a contract contains such a clause and the Commissioner does not consent to the change, but the Contractor proceeds anyway, the Commissioner may issue a Remedial Notice.
Agreement to novate should be made conditional on the new Contractor being CQC registered. The CQC may issue a sales and transfer position statement document, but this is no guarantee of registration. A provider cannot commence seeing patients until they have received their registration certificate with the regulated activities included.
5.2.3 Novation agreement – guarantee clause
There is a clause within the novation agreement covering guarantees (clause 7). The wording of this clause links the original Contractor to the new company. This means the original Contractor can be held to guarantee the behaviour and contract performance of the new company. This is a clause that is often asked to be removed or amended, especially where there is a change in those involved in the new company compared to the original contract. The wording allows you to make individual decisions for the use of this clause as it allows you to hold the original Contractor to account or not.
In all circumstances it is a local decision as to whether this clause is to be retained or not. Novation is not a right; it is at the discretion of the Commissioner so the Contractor can either accept the associated terms and conditions or stay with their current terms.
However, the Commissioner may wish to adopt the approach to hold the original Contractor to the guarantee within the original novation but allow for the removal of the guarantee if there is a further change to those in control of the company. Commissioners would need to decide about each request on a case-by-case basis, taking into consideration local circumstances.
5.2.4 Limited company to limited company
If a request is received for a change from one company to another, then this is a change in the legal entity and would be classed as a novation. The process set out in sections above will need to be followed.
5.2.5 Change in directors
A change in directors within a corporate body is not classed as a novation. The contract is held with the company. Therefore, in such instances the named directors/company officers would need to be to be reviewed for eligibility and that they meet regulations 4 and 5 for suitability. Once these checks have been undertaken and agreed a file note should be made and placed within the contract file by the Commissioner, however there is no requirement for a novation or variation.
5.2.6 Disputes
Where the Contractor does not agree with the Commissioner’s decision, the Contractor may appeal against the decision. Please refer to Chapter 13 ‘Managing Disputes’ for further information.
5.2.7 NHS dental services payment system requirements
Following the Commissioner’s decision, any changes to the contracts must be made on the relevant payment and contract management systems. Please see Annex 5.11 for further details.
6. Changes to services and finance
6.1 Introduction
Contract variations are covered in section 4.2 of this policy book.
This chapter covers where there are changes to services and changes to the payment arrangement. This includes recurrent variation to the number of UDAs to be provided under a contract (known as “rebasing”).
As decisions made in relation to the contract / agreement can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 6.1: Letters to Contractors further to request for relocation
- Annex 6.2: Re-location agreement letter
- Annex 6.3: Refusal letter for relocation
- Annex 6.4: Template Letter to Contractors proposing contract re-base
- Annex 6.5: Letter template from Contracts Manager – agreed recommended rebase
- Annex 6.6: Template letter – from Contracts Manager – agreed alternative rebase
- Annex 6.7: Template letter from Contracts Manager – last 3 year underperformance action plan
- Annex 6.8: Template letter to send out contract variation for signature
6.2 Practice mergers and/or contractual mergers
Dental practices may wish to come together in varying ways to provide support for each other, expand on the services available and/or resolve premises issues and achieve economies of scale, though contractors will have their own reasons for considering such a union.
An individual or partnership may hold more than one form of primary care contract with the commissioner and can also be a party to more than one contract. For example, a GDS contractor can also be a party under a PDS agreement and vice versa.
The underlying principles for the commissioner to consider when any such proposal is made to them are what the benefits are for the patients and what the financial implications are for the commissioner.
There are two ways in which practices may propose to merge:
a. by informal arrangements such as sharing staff which requires no change to the contracts – it is a private arrangement between the practices; or
b. by “merging” the contracts which may be done by:
- each Contractor becoming a party to the other Contractor’s contract (through variations of the contracting parties);
- terminating one of the existing contracts, continuing the other contract but varying it to include the other Contractor as a party to the contract; or
- terminating the two existing contracts and creating a single organisation or partnership which will enter into one new contract.
If one or both contracts are terminated, the relevant Contractor must give notice to the Commissioner to terminate (giving at least three months’ notice).
Merging contracts is a complex matter which should not be approached lightly by either the Contractors or the Commissioner. Adding or removing individuals or partners may be carried out in accordance with this policy but where termination is proposed, the final commissioning decision on whether contracts should be merged lies with the Commissioner. There are several important issues that would need to be considered, prior to giving consent.
a. The Commissioner should require the parties to submit a service plan to support their application, which should provide the benefits to patients and include detail on:
- how patients would access a single service;
- assurances that all patients will access a single service with consistency across provision, i.e. booking appointments, mandatory and additional services, opening hours, extended hours, and so on, single IT and phone system;
- premises arrangements and accessibility of those premises to patients; and
- proposed arrangements for consulting with the patients about the proposal, communicating the change to patients and ensuring patient choice throughout;
b. financial arrangements – the impact of directions under the SFE, or any specific terms included in the individual contracts;
c. general duties of NHS England; and
d. procurement and competition.
This is not an exhaustive list, and the Commissioner should refer to and seek appropriate guidance in each case to ensure that all relevant matters are considered.
Commissioners should advise Contractors to seek guidance from their representative bodies in this instance to ensure they follow due process and are fully aware of the implications.
6.3 Changes to services
Commissioners will need to consider changes to local service provision as a consequence of a health needs assessment of the local community with particular regard to the diverse nature of the community and reducing health inequalities in access and outcomes.
The Commissioner and the Contractor shall only agree to any change to the delivery of services after all legal obligations in respect of consultation, engagement or involvement of the public, patients and other organisations have been fulfilled.
The paragraphs below outline the principles and steps required to process the most commonly occurring service changes.
6.4 Level of services
GDS Contractors must provide mandatory services and must specify the number of UDAs to be provided by the Contractor.
If a GDS contract includes the provision of orthodontic services; the contract must also specify the number of UOAs to be provided by the Contractor.
PDS agreements are not required to provide mandatory services but such services can be included in the agreement. Where a PDS agreement includes the provision of mandatory or advanced mandatory services, the agreement must specify the number of UDAs to be provided by the Contractor.
Either party can notify the other if it believes the number of UDAs, UOAs or courses of treatment should be varied. The notice must specify the variation that the parties considered necessary and the reasons for the variation. The standard contract variation Annex 4.3 can be amended and used for this purpose.
The Commissioner may, for example, send such a notice after a mid-year review if it believes the Contractor will not achieve the number of UDAs or UOAs in the contract.
Following such notice, both parties are required to use their best endeavours to communicate and co-operate with each other with a view to determining what (if any) variation should be made to the number of UDAs or UOAs and any related variations to the agreement which may include payments to the Contractor.
Where a variation is agreed, it must be in writing and signed by both parties in order to be effective.
If the Contractor does not return a signed copy of the variation notice, then no amendment to the contract can take place.
6.4.1 Premises
A contractor may wish to make changes to its contracted premises from which services are provided.
This would likely be a significant change to services for potential service users and as such the Commissioner and the Contractor must engage in open dialogue in the first instance to consider the consequences and implications of the proposed change and discuss any possible alternatives that may be agreed between them. Failure to seek agreement with the Commissioner before a change of premises could constitute a breach and possible termination of the GDS contract or PDS agreement.
Each application needs to be dealt with on a case-by-case basis and the Commissioner should take into consideration such things as the local population’s demography, local oral health needs assessment and existing access to dentistry within the Commissioner local team’s geographical coverage as well as the overall benefit such as improvements to allow for greater use of skill mix, overall improvement in practice premises and benefits to the patient by the proposed relocation.
It is suggested that a letter is sent to the provider asking for further information as follows:
- location
- benefits to patients of the new location
- patient survey results
A template letter is provided at Annex 6.1 for ease of reference.
Canvassing patients views on the proposed move is essential to ensure that their views are captured and considered as part of the relocation process. It is suggested that practices develop a patient questionnaire as it is a legal duty to consult with patients when a change to service is proposed. A survey should be carried out by the practice for a minimum period of four to six weeks and achieve a response rate that is proportionate to the number of patients that are regularly seen.
It is important to ensure that any new premises are compliant with legislation and meet contractual clinical requirements such as HTM 01-05, infection control policies and the Equalities Act 2010 compliance and the Commissioner should consider a visit to the proposed premises to ensure they are suitable to meet the relevant requirements. This can be undertaken by the contract manager and clinical adviser.
Any new premises must receive the appropriate CQC registration to provide services before the GDS contract or PDS agreement is varied, and services provided from the new premises. The CQC will issue a sales and transfer position statement document, but this is no guarantee of registration. A practice cannot commence seeing patients until they have received their registration certificate from the CQC with the regulated activities included.
Once, and if, the final date for closure is confirmed, the Commissioner will issue a variation agreement notice to amend the registered address of the contract, and, as in other variations referred to in this policy, include the wording of the variation and the date on which it will take effect. The standard contract variation Annex 4.3 can be amended and used for this purpose. Please see attached template letter in Annex 6.2.
The Contractor will be fully responsible for cessation or assignment of the lease for any rented premises and any disposal of owner-occupied premises.
An agreement to vary the contract to include the new premises should be signed by appropriate person within the commissioning organisation. If the Contractor does not return a signed copy of the variation notice, then no amendment to the contract can take place.
The Contractor will be fully responsible for cessation or assignment of the lease for any rented premises and any disposal of owner-occupied premises.
If the relocation is refused, a template letter for use is provided in Annex 6.3.
6.4.2 Public involvement
As outlined above, it is the Commissioner’s responsibility to ensure that an appropriate public involvement exercise takes place and that any feedback from this exercise is considered before a final decision is made. This should be done in accordance with the ‘NHS England statement of arrangements and guidance for involving patients and the public in commissioning.’
Where appropriate, the Commissioner must ensure that it engages key stakeholders, including the LDC, Healthwatch, the HWB and the local council (which is likely to have an Overview and Scrutiny Committee for this purpose), discuss the feedback and ensure that this forms part of the formal application.
6.5 Financial Changes – Statement of Financial Entitlements
The contract will contain the terms of any payments due in respect of agreed services. Any change to those terms will require a notice of variation which should be provided no less than 28 days before the proposed variation takes effect.
For GDS contracts, the financial terms must reflect those set out in the GDS SFE. Any changes under the SFE should be reviewed against the terms of each of the individual contracts to ascertain what, if any, affect those changes have on local financial terms. There is no such requirement under PDS agreements where remuneration for services have been locally agreed.
6.6 Recurrent Contract Rebasing
Where a Contractor requests a permanent change to either their annual contract value or the required activity (known as “rebasing”), Commissioners should consider this request in accordance with the Regulations.
Where a Contractor has failed to achieve contract tolerance (≥96%) each year for the preceding three financial years then Commissioners should seek to reduce their annual contract value and required activity as described below.
6.7 Principles of agreeing a Recurrent Contract Rebasing
The Commissioner and Contractor will work together to mutually agree a recurrent reduction on a contract that has delivered less than 96% of their contracted UDA in the previous three financial years, where the Contractor is unable to provide adequate assurances that they are able to achieve the targeted delivery in the current financial year.
The Contractor and Commissioner should discuss historical performance, and rationale, with a view to determining what (if any) variation should be made to the number of UDA and provide sufficient opportunity for the provider to reciprocate.
The Commissioner should implement any contract variations in accordance with the relevant clause (287 and 288) of the Standard GDS Model Contract or Standard PDS Model Contract. The standard contract variation available in Annex 4.3 can be amended and used for this purpose.
Any recurrent contract rebase will usually be by mutual agreement (see section 8.4.6 on persistent under delivery). If the decision is reached to vary the contract, then the Commissioner must issue a variation notice (two copies) accordingly to amend the relevant sections of the contract / agreement. A variation notice should include the wording of the proposed variation and the date upon which the variation will take effect. The Contractor would then be required to return both signed copies of the variation notice. Once received, the Commissioner should sign both copies and return one version of the signed to the Contractor. The Commissioner should ensure that the electronically held contract documentation is amended accordingly.
Both parties should agree and have in place adequate arrangements for evaluation and review of the Contractor’s plan to ensure future delivery year on year.
As part of the local areas commissioning work plan, a review of the local needs assessment should be undertaken to determine if the proposed reductions in dental activity would be detrimental to the local population, and if a formal procurement should be undertaken to ensure there is adequate provision of primary care dentistry for the local population.
6.7.1 Data and Information to inform the discussion
A report of relevant data should be compiled to support the conversation with the Contractor, including but not limited to:
- Year-end performance data for the past three years extracted for all contracts from the ‘Contract Summary’ report provided by NHSBSA.
- Flags included in the data to enable types of contracts to be excluded from the exercise as local commissioning arrangements and/or exercise objectives require;
- Contracts with any contracted activity for Orthodontic, Sedation or Domiciliary services.
- IMOS, EDS, CDS or other specialist type contracts.
- Closed contracts.
- Contracts with any UDA reduction already agreed for the current year.
- Contracts with in-year force majeure events, whether outstanding or resolved.
- Calculations;
- To show the under delivery for each year;
- The greatest level of under delivery in the last three years and the average level of under delivery in the last three years.
The Commissioner should consider any additional exceptions such as contract variations that have taken place in the last 18 months, any Breach Notices issued and any non-recurrent changes. The Commissioner should also consider whether a contract has had a recent ownership change and whether this provides adequate assurance that the targeted delivery in the current contract year will be achieved.
6.8 Process for Implementing a Recurrent Contract Rebase
The Commissioner should send a letter to the Contractor outlining the proposed contract variations, asking for comments. A template letter for this purpose is provided in Annex 6.4 The Contractor has 14 days to respond and where the Contractor does not respond to the letter within the timescale, this should be followed up within 5 working days.
Following conversations with the Contractor (before a contract variation is issued) a letter should be sent to the Contractor confirming the contract variation. Annexes 6.5 or 6.6 provide templates for this.
The Commissioner should also ensure that the Local Dental Committee is informed as soon as this process has begun.
Where both parties agree a recurrent reduction in the contracted UDAs, the Commissioner will issue a contract variation accompanied by the relevant letter. A template letter is provided in Annex 6.8 for this purpose which asks the Contractor to confirm the changes and ask the Contractor to complete the necessary Compass Authorisation Form (CAF). The agreement reached with the Contractor needs to be monitored to ensure that any following up actions are completed, such as:
- The signed contract variation and the CAF are returned, and the entries recorded on both Compass and on any internal documentation.
To enable subsequent evaluation of the exercise all agreed contract reductions should be recorded together with a note of any other agreements or monitoring arrangements.
6.9 Non-recurrent Contract Rebasing
Any requests for non-recurrent reductions in contract value and associated activity (“non-recurrent rebasing”) received from the Contractor must be supported with evidence of exceptional circumstances and will need to be considered by the Commissioner on a case-by-case basis. The Commissioner will use the same principles and processes set out above in the sections for recurrent contract variation. Non-recurrent variation due to failure to delivery at least 30% of contracted activity by mid-year is covered under section 8.3 of this policy book.
Any non-recurrent contract variation will be by mutual agreement between the Commissioner and the Contractor. If the decision is reached to vary the contract, then the Commissioner must issue a variation notice (two copies) accordingly to amend the relevant sections of the contract / agreement. A variation notice should include the wording of the proposed variation and the date upon which the variation will take effect. The Contractor would then be required to return both signed copies of the variation notice. Once received, the Commissioner should sign both copies and return one version of the signed to the Contractor. The Commissioner should ensure that the electronically held contract documentation is amended accordingly, and the necessary updates made to the contract and payment system.
6.10 Opportunities for flexible commissioning
Opportunities for flexible commissioning in primary care dentistry: A framework for commissioners provides ICBs with an outline of the legal requirements of the national dental contractual framework, highlights the key considerations associated with procuring Additional and Further Services and provides guidance on how to ensure that contractual paperwork reflects local agreements.
This guidance supports commissioners with the following opportunities:
- Additional investment into new or existing contracts to address areas of need including;
- Increased contracting of Mandatory Services,
- commissioning additional capacity for Advanced Mandatory Services, Sedation and Domiciliary Services and Orthodontics,
- commissioning additional capacity for Dental Public Health Services and / or Further Services.
- Reallocation of existing contractual funding away from Mandatory Services into new priorities (commissioned as Additional or Further Services);
- Local negotiation of indicative rates for Units of Dental Activity (UDAs) or Units of Orthodontic Activity (UOAs).
The Commissioner must ensure that any service specification for Further Services demonstrates additionality by going beyond reasonable expectations for the provision of Mandatory Services. The Commissioner must also ensure the service does not replicate regulatory definitions of either Mandatory or Additional Services.
Commissioners are able to determine their own remuneration approaches for Further Services which could be entirely non-UDA based or take a hybrid approach where there is an overlap with Mandatory Services. Commissioners will need to ensure that any contract variation includes clear contract terms (including monitoring and recovery), and the service line is included within the Schedule 4 with separate payment terms.
Additional and Further Services may be funded in two ways: through local funds not already committed or through the redistribution of existing contract resources through an offsetting of existing UDAs.
7. Managing a PDS contractor’s right to a GDS contract
7.1 Introduction
A Contractor holding a PDS or PDS Plus agreement which is providing mandatory services, has the right to a GDS contract in accordance with regulation 21 of the PDS Regulations, which states:
“A Contractor which is providing mandatory services, and which wishes a general dental services contract to be entered into pursuant to this regulation shall notify [the Commissioner] in writing at least three months before the date on which it wishes the general dental services contract to be entered into.”
The aim of this section is to ensure that all parties to the contract understand the process and procedures that must be followed when a PDS Contractor exercises its right to transfer from a PDS agreement to a GDS contract.
Commissioners will need to ensure that its finance department and relevant persons are made aware of the change to the contracting arrangements as there will be long term financial implications. A GDS contract is not time limited and exists until terminated. Anyone with delegated authority can sign off the transfer.
The NHSBSA payment and contract management system must be updated by the officer managing the transfer and the contracts linked for payment and patient free repair and replacement purposes.
As decisions made in relation to the contract / agreement can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 7.1: PDS/PDS Plus Agreement Transfer to GDS Contract – Template Letter (Refusal mandatory services)
- Annex 7.2: PDS/PDS Plus Agreement Transfer to GDS Contract – Template Letter (Refusal eligible persons)
- Annex 7.3: PDS/PDS Plus Agreement Transfer to GDS contract – Template Letter (next steps)7.4Contract review template for transfer from PDS/PDS Plus to GDS
- Annex 7.5: PDS/PDS Plus Agreement Transfer to GDS Contract – Template letter to set up a review meeting
- Annex 7.6: PDS/PDS Plus Agreement Transfer to GDS Contract – Template Letter
- Annex 7.7: PDS/PDS Plus Agreement Transfer to GDS Contract – Template letter refusal
- Annex 7.8: PDS to GDS transfer – changes to contract payment system
- Annex 7.9: Information from NHS Resolution for requests to transfer from PDS Plus agreement to GDS contract
- Annex 7.10: Safe and Viability calculator
7.2 Notification from a Contractor
The Commissioner should receive at least three months’ notice in writing from the Contractor exercising its right to a GDS contract.
The Contractor’s notice must:
- state that the Contractor wishes to terminate the PDS agreement;
- state the date on which the Contractor wishes the PDS agreement to terminate which must be at least three months after the date of service of the notice;
- give the name of the person(s) with whom the Contractor wishes the Commissioner to enter into a GDS contract (a person’s name may only be given in a notice if that person is a party to the PDS agreement); and
- confirm that the person(s) so named meet the conditions set out in section 102 of the NHS Act and regulations 4 and 5 (where applicable) of the GDS Regulations or, where the Contractor is not able to confirm, the reason why it is not able to do so and confirmation that the person or persons immediately prior to entering into the GDS contract will meet those conditions.
7.3 Process for PDS Agreements
The Commissioner must acknowledge receipt of the notice within seven days beginning on the day it received the notice.
The Commissioner will check that all relevant and necessary information has been provided in the Contractor’s notice and undertake a review of the PDS agreement to:
- establish if the Contractor provides mandatory services; and
- check if they are eligible to hold a GDS contract (as set out in section 102 of the NHS Act persons eligible to enter into GDS contracts) and regulations 4 and 5 of the GDS Regulations and described in Chapter 3.
If the Contractor does not provide mandatory services, the Commissioner must notify the Contractor that they are not entitled to transfer to a GDS contract. A template letter is provided in Annex 7.1.
If the Contractor is not eligible to hold a GDS contract the Commissioner must refuse to enter into a GDS contract. A template letter is provided in Annex 7.2.
If the Commissioner confirms that the Contractor provides mandatory services and is eligible to hold a GDS contract under section 102 of the NHS Act and regulations 4 and 5 of the GDS Regulations, the Commissioner will acknowledge receipt of the notice and outline the next steps within seven days of receipt of the notice. A template letter is provided in Annex 7.3.
Unless agreed otherwise by both parties the new GDS contract will require provision of the same services as were provided by the Contractor immediately prior to the PDS agreement terminating. For activity this is the same number of UDAs for mandatory services, and (where commissioned) the same number of UOAs for orthodontic services. For other services such as sedation services or domiciliary services it is the same number of courses of treatment as specified in the PDS agreement. This does not preclude the Commissioner negotiating a revised contract value for the new GDS contract.
The Contractor will be entitled to a Negotiated Annual Contract Value (NACV) for the GDS contract as set out in the GDS SFE. The Commissioner and the Contractor must agree, in respect of the first financial year during which a GDS contract has affect a NACV for the GDS contract, based on the number of units of dental activity and, where applicable, orthodontic activity that the Contractor is required to provide under its GDS contract.
The Commissioner has the right to consider and negotiate the average value of the units of dental and orthodontic activity that it commissions from the Contractor. This position has been confirmed by the Family Health Services Appeal Unit (FHSAU) (now NHS Resolution) case number 15189 (August 2009). The activity and services must remain the same as they were under the PDS agreement unless agreed by both parties, but the indicative UDA (and if applicable UOA) rates may be negotiated.
On receipt of a notice exercising the right to transfer to a GDS contract, the Commissioner shall undertake an internal review of the PDS agreement. The Commissioner will access benchmarked data (including, for example, indicative UDA values, NICE recall guidance adherence and patient access data) from NHSBSA to enable them to determine whether a PDS agreement is providing value for money and performance in terms of activity and compliance.
The Commissioner will negotiate the NACV to bring the Contractors in line with the average local UDA/UOA rates. Annex 7.4 contains a contract review template that should be considered. The Commissioner may at its discretion negotiate a decrease or an increase to the indicative UDA/UOA rate for example, in reasonable and appropriate circumstances such as if the Contractor is a financial outlier and such decrease will seek to ensure that the service remains safe and viable.
The Commissioner will offer the Contractor, in writing, a meeting to discuss the NACV offer being made to them in view of the contract review. A template letter is provided in Annex 7.5.
During this period of negotiation, the Contractor may wish to issue a counteroffer for consideration. Once the negotiation period has been completed the Commissioner will provide a final offer confirmed in writing.
If the Contractor agrees the new NACV, this will be confirmed in writing, a date for the termination of the PDS agreement will be agreed and a new GDS contract issued with a start date immediately following the termination of the PDS agreement. The termination of the PDS agreement and commencement of the GDS contract should be on the date provided in the notice from the Contractor exercising its right to a GDS contract unless a different date is agreed between the parties. A template letter is provided in Annex 7.6.
If the Contractor does not agree the new NACV, the Commissioner cannot agree to transfer the PDS agreement to a GDS contract. The Contractor must be informed of their right to dispute the decision under regulation 21(9) of the PDS Regulations. A template letter is provided in Annex 7.7.
Following the agreement to transfer the PDS agreement to a GDS contract the Commissioner must update the NHSBSA payment system. Details are contained in Annex 7.8.
The Contractor may at any point choose to withdraw their application to transfer to a GDS contract and continue with their current PDS agreement should agreement not be reached on the NACV for the GDS contract.
Where a GDS contract commences on a day other than 1 April the Contractor must provide, during the remainder of that financial year, any UDAs or UOAs and any courses of treatment including the provision of sedation or domiciliary services the Contractor would have been obliged to provide or contribute to immediately before the GDS contract begins.
7.4 PDS Plus Agreements and Non-Standard PDS Agreements
PDS Plus agreements and other non-standard PDS agreements are regulated by the PDS Regulations and Contractors have the same right to transfer to a GDS contract. Where a notice to transfer a PDS Plus agreement or non-standard PDS agreement is received the Commissioner should acknowledge receipt of the request.
The process above should be followed but should also include compliance with any terms of the PDS Plus agreement which govern the transfer to a GDS contract (for example, paragraph 2.5 of Schedule 3 of the DH Standard PDS Plus Agreement states):
“In the event that the Contractor exercises its right to a GDS contract the contract value that will be negotiated as the NACV will be based on the payments that are made under the SFE. For the avoidance of doubt the payment made under the SFE is the services payment”. The “services payment“ is considered the total contract payment NOT just that paid for the services element of a PDS Plus contract.
This clause means that the contract value must be guaranteed as part of the transfer, but the Commissioner has the right to negotiate the activity level under the new contract.
The minimum service activity of a PDS Plus agreement may have been procured at a higher level than 51% of the total PDS Plus agreement value.
Further to a recent litigation case, NHS Resolution indicated that a safe and viable offer needed to be agreed by both parties. Further information from NHS Resolution and a calculator to determine a safe and viable rate is provided in Annexes 7.9 and 7.10.
7.5 Disputes
Where there is a dispute about whether a person satisfies the conditions set out in section 102 of the NHS Act or regulation 4 or 5 of the GDS Regulations, the Contractor may appeal to the First-tier Tribunal.
Any other dispute relating to the GDS contract shall be determined by the Secretary of State (NHS Resolution) in accordance with regulation 8(3) and (4) of the GDS Regulations (pre-contract disputes).
Further information can be found in Chapter 13 – ‘Managing Disputes’.
8. Financial recovery and reconciliation
8.1 Introduction
This section provides guidance on the management of the mid-year and year-end financial reconciliation and recovery process for all dental contracts.
The policy covers all GDS and PDS Contractors regardless of their legal entity.
The Commissioner will need to ensure that, where there are any adjustments that are made to dental contracts, reclaimed money will need to be logged and superannuation reclaimed. Any variation of contract that takes place will also need to be accounted for, as this may affect the recurrent financial obligations placed upon the Commissioner.
The NHSBSA Dental Services team (NHSBSA) payment and contract system also needs to be updated by the officer managing the processes as this will affect contractual payments to Contractors.
As decisions made in relation to the contract/agreement can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
This section describes the contractual and regulatory processes required to:
- review activity at both mid-year and year end;
- make the required financial recovery; and
- issue a Breach Notice, in line with requirements as set out in paragraph 73 Part 9 of Schedule 3 of the GDS Regulations, and the same provision in the PDS Regulations.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 8.1: National Dental Contract Management Single Operating Model Mid-year and Year End Timeline
- Annex 8.2: Template National Dental Contract Management Service Mid-year Review Letter
- Annex 8.3: Template National Dental Contract management Service Mid-year SMART Action Plan template
- Annex 8.4: Template national Dental Contract Management Service Mid-year Review Complete template letter
- Annex 8.5: Template National Dental Contract Management Service Mid-year November withhold template letter
- Annex 8.6: Template National Dental Contract Management Service Mid-year January withhold template letter
- Annex 8.7: Template National Dental Contract Management Service Mid-year Release withhold template letter
- Annex 8.8: Template National Dental Contract Management Service Year-end Letter
- Annex 8.9: Breach Notice – Year end
- Annex 8.10: Year-end under delivery – less than four percent under-delivery – exceptional circumstances
- Annex 8.11: Letter to Contractors to request KPI information
- Annex 8.12: KPI calculator
8.2 National Dental Contract Management Service – operating model and principles
NHSBSA, on behalf of Commissioners, will deliver the year end reconciliation and mid-year review of those dental contracts where activity is remunerated via Compass.
Details of delivered activity is submitted by Contractors to NHSBSA who verify all claims then hold this data via Compass.
All outcomes from the year end and mid-year reviews (carry forward of activity and/or recovery of monies) will be administered by NHSBSA via Compass.
The Single Operating Model (SOM) details NHSBSA operational delivery. The SOM provides a framework for the delivery of year end reconciliation and mid-year review. Commissioners are permitted to deviate from the model to consider local circumstances.
With reference to appropriate regulation, terms of the standard dental contract and agreement (GDS / PDS) and best practice, dental contracts are subject to a year end reconciliation and mid-year review of delivery against contracted activity.
8.2.1 Timeline
A generic timeline with key milestones for both year end and mid-year can be found in Annex 8.1. NHSBSA will update this annually for Commissioners.
8.2.2 Categorisation
In line with the standard operating model, contracts will be categorised as either 1,2 or 3 having considered the following criteria.
- The quality of the contract data held in Compass in relation to the contract’s (and any subcontracts, if appropriate) delivery targets.
- Any other or ongoing commissioning considerations relating to previous delivery of the contract.
Commissioners will retain responsibility for categorising contracts in their ICBs.
- Category 1: Details recorded in Compass by the Commissioner are up to date and accurate and NHSBSA can complete the year end and mid-year activities based on these.
- Category 2: Details recorded in Compass by the Commissioner require additional information to complete the year end and mid-year activities, which will be supplied to NHSBSA by the Commissioner.
- Category 3: Retained by the Commissioner for local management and resolution.
All GDS, PDS and PDS Plus contracts will be considered as either category 1 or 2 by default.
Where a Commissioner retains a contract in category 3 for local resolution, either prior to or during the mid-year and/or year-end process, it remains the responsibility of the Commissioner to complete any actions required to resolve the relevant process.
This includes, but is not limited to, obtaining action plans for contracts delivering less than 30% at the mid-year point, withholding of in-year contractual payments where necessary, completing a full year end reconciliation, ensuring carried over activity and/or financial recovery/payment is administered appropriately via Compass and resolving any Contractor queries. It is recommended that Commissioners follow the same timeline and templates used by NHSBSA for category 3 contracts.
There are established points throughout the process for reviewing the categorisation of contracts which may include category 3 contracts being revised to category 1 or 2 and/or vice versa.
8.2.3 Communication
Commissioners will regularly receive updated spreadsheets from their case worker which will provide a summary of activity undertaken on all contracts This will be used as sign off mechanism and act as an audit trail of any decisions made. Commissioners may also use and share this with finance teams to prepare for monthly and year end accounting for over and underperforming dental practices.
All further correspondence with Contractors (and/or appropriate practice and body corporate team members) will be via a secure email address by default in the first instance.
NHSBSA will use Compass to issue contractual correspondence available to both Commissioners and Contractors.
8.2.4 Query management
All queries from Contractors/communications relating to category 1 and 2 contracts remain the responsibility of NHSBSA; Commissioners are advised to sign post enquires to NHSBSA unless they relate to category 3. NHSBSA will send an automatic holding email to acknowledge the receipt of any query.
8.3 Mid-year review
The obligation for mid-year reviews is set out in paragraph 58 of Schedule 3 of the GDS Regulations and the same provision in the PDS Regulations.
The Commissioner will review the categorisation of contract details recorded in Compass prior to the mid-year report publication with reference to 8.2.2.
The Commissioner will provide details to NHSBSA for category 2 contracts that allow for the completion of mid-year delivery (including, but not limited to, ‘parent/child’ details for sub-contracts/incorporations/mergers/closures, force majeure, payments more than contract). Categorisation should be completed, and information provided in time for category 2 letters by mid-October.
By 31 October in each financial year NHSBSA must, on behalf of the Commissioner, determine the number of UDAs and UOAs that the Contractor has provided between 1 April and 30 September in that year. This information will be based on the notifications of treatment (FP17s) made by the Contractor under paragraph 38 of Schedule 3 of the GDS Regulations and paragraph 39 of Schedule 3 of the PDS Regulations and provided to the Commissioner by NHSBSA.
Where the notifications of treatment are disputed by the Contractor, the Contractor should liaise directly with NHSBSA to resolve queries.
Delivery of contracted activity is not considered to commence until a Contractor has delivered activity brought forward from the previous contractual year. Delivery of brought forward activity will be reviewed at the mid-year point and will not contribute to the 30 percent.
Notifications of courses of treatment must be made within 2 months of a course of completed treatment. Contractors must ensure that notifications are made on time as the Commissioner is not obliged to pay for activity which is not notified in accordance with this 2-month deadline.
Where the Contractor has provided more than 30% of the required activity in that financial year (between 1 April and 30 September) NHSBSA will send a letter to the Contractor and a mid-year meeting may not be required.
Where the Contractor has provided less than 30% of the required activity in that financial year (between 1 April and 30 September) the Commissioner must:
- notify the Contractor regarding the activity provided under the contract in the first half of the year;
- set out the number of UDAs and UOAs that the Contractor has provided together with the percentage total of the total number of UDAs and UOAs that this represents; and
- formally require the Contractor to participate in a mid-year review of its performance in relation to the contract. Failure by the Contractor to engage must be evidenced and formally communicated to the Contractor together with the implications of non-engagement
- A mid-year review meeting does not necessarily need to be face-to-face and can be conducted on the telephone, or virtually if appropriate but must be recorded.
8.3.1 Mid-year letter
NHSBSA will upload a mid-year letter (Annex 8.2) onto Compass for all category 1 and 2 Contractors outlining their delivery against contracted activity submitted for inclusion in the September schedule.
An email will be sent to all Contractors highlighting that the letter has been uploaded and can now be accessed.
The Commissioner is responsible for confirming the position to the NHSBSA for any category 3 Contractors who will then upload reports onto Compass outlining their delivery against contracted activity submitted for inclusion in the September schedule.
8.3.2 Mid-year review meeting
This meeting does not necessarily need to be face-to-face and can be conducted on the telephone, or virtually if appropriate but must be recorded.
Where the Contractor provides evidence or reasonable explanations and/or remedies at the review meeting, the Commissioner may take no further action following the mid-year review. The Commissioner should be satisfied that the Contractor is on target to deliver the contracted activity by the year end. At the mid-year review meeting the Commissioner and the Contractor shall discuss:
- Any written evidence the Contractor put forward to demonstrate that it has provided a higher number of UDAs and UOAs during the first half of the financial year than the Commissioner has indicated; and
- Any reasons the Contractor provides for the level of activity in the first half of the financial year.
Where, having taken into account any evidence or reasons put forward by the Contractor at the mid-year review (e.g. as a result of a force majeure event) and the Commissioner nevertheless has serious concerns that the Contractor is unlikely to provide the number of UDAs or UOAs that are required by the year end, the Commissioner must seek to agree a non-recurrent reduction of contract value and associated delivery requirements.
- Produce an in-year contract variation within 14 days of the mid-year meeting
- Amend Compass payment system within 5 days of receipt of signed variations.
The Commissioner and the Contractor may agree at any time to vary the contract to adjust the number of UDAs or UOAs to be provided under the contract and the monies to be paid to the Contractor under the contract. Either the Commissioner or the Contractor can notify the other party of its need for a variation, specifying why this is necessary. The parties will use their best endeavours to communicate and co-operate with each other to agree what (if any) variation should be made and the related variations to the contract. No amendment or variation to the contract will have effect unless it is in writing and signed on behalf of the Commissioner and the Contractor.
Process for the Commissioner to follow:
- send a letter asking the Contractor to arrange a review meeting;
- hold mid-year review meeting;
- follow up the mid-year review meeting:
- a final copy of the notes of the meeting should be sent to the Contractor;
- if the Commissioner is still concerned about contracted delivery, it mayrequest the Contractor to comply with a written plan drawn up by the commissioner to ensure that the level of activity during the remainder of the financial year;
- the Commissioner may withhold any monies as appropriate and make any adjustments to the payment system in accordance with paragraph 59(2) and (3) of Schedule 3 of the GDS Regulations and the same provision of the PDS Regulations;
- Send a written copy of the review and any feedback from the action plan to the Contractor.
8.3.3 Withholding payments following a mid-year review
If a Commissioner fails to agree in year contract variation and remains unassured that the Contractor will deliver the level of activity during the remainder of the financial year the Commissioner may withhold monies in line with paragraph 59 (3) of Schedule 3 of the GDS Regulations and the same provision of the PDS Regulations. The maximum amount that may be withheld is:
- the amount that is payable under the contract in respect of the number of UDAs or UOAs required to be provided in a financial year;
- less the amount that would be payable under the contract as a relevant proportion of that amount if the Contractor provided in the whole of the financial year only twice the number of units of dental activity or orthodontic activity that was provided between 1 April and 30 September.
Where the Commissioner withholds monies, it shall ensure that it pays the withheld monies to the Contractor promptly following the end of the relevant financial year where the Contractor has:
- provided the contracted UDAs and UOAs; or
- has failed to provide the contracted UDAs or UOAs but has delivered 96% of above of their contracted activity
Delivery will be reviewed after the February schedule through to the May schedule and any withheld payment will be paid to Contractors on the next available payment date after delivery of their contracted activity is confirmed. A template letter is available for this purpose in Annex 8.7, otherwise this will be included in the final year end calculation.
8.4 Year-end reconciliation – GDS, PDS and PDS Plus
The Commissioner will carry out a year end reconciliation on all primary care dental contracts to ensure activity is being delivered against contracted requirements.
In June of each financial year, NHSBSA will provide Commissioners with contract level data detailing the actual level of dental activity which has been delivered during the previous financial year.
This figure is the total of the notifications sent by the Contractor to NHSBSA by way of FP17 submissions on completed courses of treatment.
The Commissioner will use data supplied by NHSBSA in relation to the total of the notifications received (the total number of UDAs and UOAs). The Contractor is responsible for providing written documentation and evidence of any dispute with the NHSBSA data and any outcome to the Commissioner’s primary care dental lead to take into consideration.
While the contract holder should aim to deliver 100% of their total contracted units of activity, there will be deviations which must be dealt with as set out below.
NB: Rounding up or down of year end performance figures is prohibited.
It is recognised that at times manual adjustments need to be made to the NHSBSA data. This can be because of:
- Missing claims (Contractors are required to submit electronically to support any manual post end year statement publication changes);
- Exceptional circumstances (as defined in section 8.4.9 of this policy book with examples in Annex 8.10);
- Change of ownership which requires contract figures to be combined at year end.
Where any amendments are made, they should be highlighted on the year end spreadsheet and signed off by the appropriate signatory e.g. Senior Contract Manager and / or Senior Finance Manager who must be independent from the individual who has calculated the amendment.
From an audit perspective, Commissioners should undertake a quarterly reconciliation of NHSBSA data. This will enable Commissioners to identify any anomalies or exceptions in a timely manner and discuss any issues with practices.
8.4.1 Year end reconciliation categorisation timeline
Commissioners will categorise contract details recorded in Compass prior to the year-end letter publication.
Commissioners will provide details to NHSBSA for category 2 contracts that allow for the completion of year end delivery (including, but not limited to, ‘parent/child’ details for sub-contracts/incorporations/mergers/closures, force majeure, payments more than contract).
Commissioners should aim to have categorised all contracts and sent through the required information for category 2 contracts by mid-May otherwise they will automatically be classed as category 3 and will remain with Commissioners to resolve.
NHSBSA will make all year-end adjustments to category 1 and 2 contracts in Compass.
8.4.2 Year-end review letter
NHSBSA will upload an individual year end letter onto Compass for all category 1 and 2 Contractors outlining their delivery against contracted activity in the preceding financial year. A template letter is available for this purpose in Annex 8.8.
An email will be sent to all Contractors highlighting that the letter has been uploaded and can now be accessed.
8.4.3 Under delivery of UDAs or UOAs – below 96%
Where a Contractor has delivered less than 96% of their contracted activity, the Commissioner will recover the full amount of money (the overpayment to the Contractor in respect of the activity delivered under the contract) up to the full contract value.
Financial recovery will be administered by NHSBSA and will routinely be via three instalments of deductions from September to November’s scheduled payments (inclusive).
Any requests to extend instalments beyond this will be forwarded to the Commissioner for consideration. NHSBSA will retain responsibility for administering the agreed instalment plan in Compass once agreed by the Commissioner.
The maximum length of a repayment plan is the end of March following the review date unless the Commissioner supports the Contractor’s grounds for additional time to make the recovery.
Where a repayment plan is agreed, the Commissioner will need to consider Patient Charge Revenue charges, superannuation, and levies etc., to ensure there is enough money in the scheduled payment to cover the debt. A repayment plan minimises the financial risk to the Commissioner and should ensure that it does not allow the Contractor to go into negative payments, therefore creating a further cumulative debt. The repayment plan should be agreed in writing between the Commissioner and the Contractor and signed by both parties.
The Commissioner can agree a mix of a lump sum payment and a repayment plan for the balance.
The preferred repayment mechanism is through the NHSBSA Compass system.
Where a variation to the contract is agreed, adjustments should also be made on the payment system. Any contractual variation of the contract must be agreed by both parties (the Commissioner and Contractor) unless in relation to persistent under delivery of contracted activity covered within section 8.4.6 of this policy book. Further information can be found in Chapter 6 ‘Changes to Services and Finances’ in the Contract Rebasing section.
8.4.4 Breach Notices
In addition to recovery of the overpayment, NHSBSA may, on behalf of the commissioner, also serve a Breach Notice to the Contractor for failure to deliver the contracted activity. A template Breach Notice is available in Annex 8.9. The Commissioner will have regard to the reasons for under-delivery including those covered by the circumstances in Annex 8.10.
NHSBSA will prepare a list of contracts delivering under 96.0% of contracted UDAs and/or UOAs and/or less than 100.0% of other additional services and further services which the Commissioner will be required to review in order to decide which contract should receive a Breach Notice. NHSBSA will communicate with Commissioners to then ensure all Breach Notices are dated, printed, and signed off by the appropriate person within the commissioning organisation.
Issuing of Breach Notices will be the responsibility of NHSBSA after communication with Commissioners. All Breach Notices will be available on NHSBSA Compass system.
If either of the following circumstances occurs and the time of the relevant circumstances has elapsed, the Commissioner shall act as though the Breach Notice was not issued. The Commissioner will not look to rely on the Breach Notice when taking any future actions under the GDS contract or PDS agreement:
- A Breach Notice is issued to a Contractor who has achieved between 90 percent and less than 96 percent of a contract’s UDA/UOA target in a particular financial year, and, in the following two financial years, the Contractor achieves 96 percent or more of the contract’s UDA/UOA target.
- A Breach Notice is issued to a Contractor who has under-delivered against the contract’s UDA/UOA target in a particular financial year and, in a following year, the Contractor and Commissioner agree a recurrent rebase of the contract’s UDA/UOA target.
For more information on Breach Notices outside of the year-end review process see Chapter 10.
8.4.5 Delivery within tolerance of UDAs or UOAs – between 96% and 100%
Where the Contractor fails to deliver the full contracted UDAs or UOAs, and where this amounts to 4% or less of the total contracted UDAs or UOAs, and the Contractor agrees to provide the units it has failed to deliver within a period of no less than 60 days and agrees to an extended time period with the Commissioner, the Commissioner will not take any financial action for failure to provide the contracted UDAs or UOAs. This is set out at regulation 18 of the GDS Regulations and Regulation 15 of the PDS Regulations.
If a contract under-delivers within the tolerance level, then this activity must be delivered within the first 60 days of the next financial year. Any carry forward of activity must be entered onto the payment system.
Breach Notices in relation to the under delivery of UDAs or UOAs cannot be issued if a Contractor delivers activity within this range.
8.4.6 Contract variation following persistent under-delivery
Where a Contractor has delivered less than 96% of their annual contracted activity over a period of three consecutive years (definition below) Commissioners should in the first instance seek to agree a recurrent reduction to the annual contract value and associated delivery as determined in the statutory instrument 2023 No.554 .
In the event that a Contractor has agreed with their Commissioner a non-recurrent rebasing for any single year, this temporarily revised contract value would not exclude that year from consideration for a longer-term rebasing, where 96% of the underlying contract activity had not been delivered. If the non-recurrent rebasing was agreed because the Contractor had exceptional circumstances then that year would be excluded but not break the continuity of three financial years.
Commissioners should assess performance over the course of the relevant 3 consecutive years and re-base the contract at the highest level across those 3 years. Where this agreement cannot be reached then the Commissioner has the ability to take unilateral action to recurrently reduce the annual contract value and associated activity as an alternative to contract termination. To proceed with a unilateral reduction to the annual contract value and associated activity the Commissioner must be able to demonstrate the following:
- that the Contractor has failed to achieve the activity levels required for contract tolerance in the preceding 3 years which will exclude activity during the pandemic years defined as: 1 April 2020 – 31 March 2021 and 1 April 2021 – 31 March 2022.
Qualifying periods for calculation are defined as: 1 April 2019 – 31 March 2020 and any years from 1 April 2022 onwards and must ensure that there have been no exceptional circumstances as per the Policy Book for Primary Dental Services ( 8.4.9 in the policy book, and where exceptional circumstances apply this year should not be taken into account).
The Commissioner must be able to evidence that:
- they have attempted to hold an annual or mid-year review with the Contractor for each year of under-performance
- the Contractor has been issued with breach notices in each year of under-performance
- that they can evidence that they have been unable to reach a mutual agreement on a reduction in the annual contract value and associated activity
All contract variations will take effect from the beginning of the following financial year and the Contractor will then be assessed on the new level of contracted activity going forward.
Where a Contractor disagrees with the decision, they would be expected to exhaust local contract dispute resolution before referring the matter to NHS Resolution.
8.4.7 Under delivery of domiciliary and sedation services
Where the Contractor is contracted to provide domiciliary and/or sedation services the contract must specify the number of courses of treatment the Contractor is required to provide or contribute to as a referral service.
Where the Contractor fails to provide the contracted number of courses of treatment the Commissioner may serve a Breach Notice to the Contractor.
Where the contract details the financial sum payable in respect of the domiciliary and sedation services and these are not provided by the Contractor in the relevant financial year, the Commissioner may seek recovery for the overpayments.
8.4.8 Over delivery
Unless the contract specifies that the Commissioner will pay for the delivery of UDAs or UOAs over the contracted activity set out at clauses 77 and 78 of the standard GDS contracts and PDS agreements there is no requirement for the Commissioner to make additional payments to the Contractor or to take this activity into account during the next financial year. The Commissioner may allow a tolerance of up to two percent of UDAs or UOAs per year (therefore a maximum of 102% of the contracted UDA/UOA activity). The Commissioner may pay for the additional activity, or it may be credited to the following contract year.
Under Primary Dental Services Statements of Financial Entitlements (Amendment) Directions 2018, section 10A the Commissioner may allow for carry forward/payment up to 104 percent of UDA and/or UOA activity delivered under pre-approved oral health programmes.
In addition, where Commissioners have the resources and where they have reached agreement with the Contractor, by way of a contract variation, Contractors will be able to deliver up to 110% of their actual contracted UDA/UOA activity. Any provision to deliver up to 110% is in year and is not a permanent variation to contract value.
Commissioners will, where relevant, run a transparent process to identify Contractors with a credible plan to deliver additional capacity and invite them to apply for additional funding up to 110% via an expression of interest process. This process should include evidence of previous year’s performance and an overview of the areas they expect to be able to use additional funding assessing previous year’s performance and award funding on the basis of population need and inequalities.
If a Contractor wishes to carry forward over delivered activity (up to 2%) instead of receiving a full payment then it will be at the Commissioners discretion to consider the appropriateness of the individual circumstances as part of the decision making process.
The Commissioner has the discretion to commission non-recurrent activity in any financial year which may be funded according to local priorities and circumstances.
The process map below shows the process that Commissioners should go through for Contractors to access additional funding:
8.4.9 Exceptional Circumstances
In exceptional circumstances, there may be instances in which a contract holder is unable to fulfil its contractual requirement to deliver the contracted activity. These cases need to be considered on an individual basis and could include a decision by the Commissioner to waive its rights to recover overpayments where agreement is reached on how the activity will be delivered or may agree to the overpayment being repaid over a longer period than that set out above.
For further information please refer to Chapter 14 – ‘Adverse Events’. Annex 8.10 contains a table of some elements which could be considered exceptional circumstances, subject to the provision of supporting evidence. This list is not exhaustive.
8.4.10 Late Submission of online FP17
Where a Contractor has submitted a claim two months later than the completion date this will be deemed as a late submission and zero UDAs will be allocated but will still be processed for patient charge revenue.
Where a Contractor has a query around being entitled to the UDAs, they should contact NHSBSA providing the following:
- Provider number;
- Performer number – this helps if it is a Corporate Body;
- Correct pay statement; and
- Patient name and date of birth and/or claim reference number
NHSBSA will investigate if there has been a NHSBSA act, error or omission and provide a recommendation to the Commissioner. The final decision remains with the Commissioner.
If investigations show that the Contractor is entitled to UDAs an override rule may be applied on the contract to allow the claims to re-processed.
If an override rule is created, electronic claims can be re-sent under a Schedule Query Indicator and online claims can be amended in Compass. If the year-end report has already been generated the claims cannot be amended as above; instead, NHSBSA working with the commissioning team will either amend the Contractor’s annual contracted UDA target or agree not to carry over part/all the Contractor’s UDA shortfall.
If the late submissions are not allowed the Contractor is entitled to appeal against the decision.
8.4.12 PDS Plus
The Commissioner will follow both the mid-year and year end procedures set out above, in line with the PDS Regulations and SFE for any PDS Plus agreements.
Schedule 3 of the PDS Plus agreement provides the breakdown of agreement values into service payment, access payment and performance payment.
All payments are paid monthly and paragraph 8 of Schedule 3 of the PDS Plus agreement outlines the annual reconciliation for the service, access, and performance payments. Commissioners will need to calculate any under performance in line with the details contained within each specific PDS Plus agreement.
Where PDS Plus agreements contain KPIs, Commissioners must request evidence from providers to confirm the KPIs have been met. This information should be sent by providers annually and be managed as part of the year end process. Information must be submitted by providers no later than 30 June each year. A template letter is attached for the information request in Annex 8.11.
Commissioners should review the KPI evidence and factor their achievement into the overall year end calculations of the provider. A sample template is provided in Annex 8.12.
The Commissioner should share the findings with the provider to agree the year end position.
9. Orthodontics
9.1 Introduction
This policy covers specific issues in relation to the management of orthodontic contracts including:
- the management of a second course of treatment;
- orthodontic transfers from abroad; and
- orthodontic close down arrangements.
As decisions made in relation to the contract and its applications can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 9.1: Template letter for patients from overseas requesting NHS orthodontic treatment
- Annex 9.2: Orthodontic pathway with overall costs
- Annex 9.3: Template Capture Form for Completion by Contractor
- Annex 9.4: Orthodontic Close Down Payment Template
- Annex 9.5: Template PDS variation document
9.2 Second course of treatment
Detailed information on commissioning orthodontic services can be found in the Guide for Commissioning Dental Specialities: Orthodontics
The commissioning guide, page 12 point 4.4.1 states:
Patients will only be offered one course of NHS-funded routine Orthodontic treatment, unless there are exceptional circumstances. Such cases include where interceptive or growth dependent treatment has been undertaken and IOTN remains greater than 3.6. Any patient not meeting these circumstances would need to apply via their Commissioner who will seek clinical advice from either their dental LPN or MCN to approve a second course of treatment. There may be occasions when an appliance has to be removed during a course of treatment to allow a patient to undergo other procedures such diagnostic services. Recommencing treatment would not constitute a new course of treatment.
Where a patient has been refused a second course of orthodontic treatment and has appealed this decision, Commissioners need to ensure there is a local process for patients to appeal.
9.3 Orthodontic transfer from abroad
Where a patient begins treatment abroad (not just EEA) and subsequently becomes a permanent resident in the UK and entitled to NHS care, NHS criteria is applicable and not the criteria from the country where they began treatment.
Patients should arrange for their original patient records including study models, x-rays, photographs and notes to be provided so that an NHS orthodontic specialist who is calibrated in IOTN can confirm whether they would have met NHS criteria on their original assessment date (i.e. that they were under 18, an IOTN of at least 3.6 and have good oral health).
Please see attached draft template (Annex 57) that can be amended for use.
If the orthodontist feels that the NHS criteria would have been met, a course of treatment can be provided.
If the orthodontist does not feel that the NHS criteria would have been met, a course of treatment will not be provided.
Any children with a device in situ, unable to access dental records, pictures, and study models, should be assessed by an NHS orthodontic specialist who is calibrated in IOTN. Patients may self-refer directly to an orthodontic practice or referral may be made via high street dental practices. If following this assessment, the child is deemed eligible for continuation of NHS treatment they will need to have their treatment continued in the same way (and to the same timescales) as others who are already in treatment, and therefore seen ahead of any patients on waiting lists.
In line with the Regulations, Contractors will be able to claim for a case start for each patient deemed eligible for treatment via submitted FP17O claim forms. Renumeration for these cases will attract the appropriate number of Units of Orthodontic Activity (UOAs), as set out in the dental Regulations.
If, following any such assessment a child is deemed ineligible for NHS orthodontic treatment, and where parents or carers have confirmed they are unable to self-fund completion of a private course of orthodontic treatment, children can be debonded by a local NHS orthodontist. The Contractor will be awarded 1 UOA. At the time of publishing this policy booklet, we are working with the NHSBSA for the additional of a further field to be added to the electronic FP17O claim form that captures Assessment and De bond – Overseas patient. Contractors will be able to make a claim for debonding patients via an FP17O form and once available will be able to submit retrospective claims from 1 October 2022.
Adults are not usually eligible for NHS funded orthodontic treatment. Any adults arriving in England with an orthodontic device in situ who seek dental care should be made aware that treatment is not provided under NHS contracts and that they will need to access ongoing orthodontic care privately. They should also be advised of the clinical risks associated with leaving any active devices in situ. If a patient is charge exempt they may be offered debonding of their device under an NHS orthodontic contract in order to mitigate any associated clinical risks. In these circumstances, 1 UOA will be credited to the orthodontist’s contract. and again, at the time of publishing this policy booklet, we will work with NHSBSA for the additional of a further field to be added to the electronic FP17O claim form that captures Assessment and De bond – Overseas patient.
9.4 Orthodontic close down arrangements
9.4.1 Introduction
This section describes the agreed set of principles to manage close down arrangements following the re-procurement of an existing orthodontic contract.
These principles may also apply in the following circumstances:
- where a Contractor plans to retire or terminate their contract for personal reasons, and there is no current agreement from them to complete patients in treatment;
- where a Contractor plans to retire or terminate their contract for personal reasons, and there is no identified commissioning need to re-procure services;
- in the event of the sudden death of the Contractor (who is an individual contract holder) where the representatives of the Contractor are willing and able to ensure completion for patients in treatment
Where Contractors are not willing to agree with close down arrangements, all patients, those on a waiting list for assessment and or treatment, and those in active treatment, will need to transfer to a new Contractor and continuation of treatment or a full course of treatment provided, subject to eligibility criteria.
The close down arrangements where applicable include:
- a process for validating the patient list from the existing Contractor;
- calculation of close down payments to be made to the existing Contractor to complete patients in active treatment;
- contract documentation required to accompany close down payments
9.4.2 Agreed approach for close down arrangements
The following principles should be applied to close down arrangements:
- One approach is to be applied across NHS England to manage patients affected by contracts in transition and to identify patients in active treatment;
- It is in the best interest of the patient to complete their course of orthodontic treatment with their existing provider and the Commissioner should approach the current Contractor as early as possible to discuss the close down arrangements;
- A one-off close down payment will be paid to the Contractor to complete outstanding courses of treatment;
- The payment to Contractors will be based on the number of patients in active treatment, split into two categories:
- Patients under active treatment – with a fixed or removable appliance;
- Patients under supervised retention;
- The payment for active treatment only covers those patients who are being treated using fixed appliances; it should not be used for patients who are being treated using removable appliances;
- A one-off fee of £126 will be paid for patients in active treatment with a removable appliance;
- Patients who are deemed on the waiting list, have had case assessment only or have a removable appliance will be managed separately to this process and most likely by a new Contractor;
- A one-off fee of £662 per patient will be paid for those patients in active treatment. This value is based on 50% of the cost of a course of treatment at national average UOA value of £63 (21 UOAs * £63). This one-off fee is payable for all patients in active treatment irrespective of the stage of treatment they are at. It is recognised that there will be a combination of patients at different stages of their treatment;
- A one-off fee of £25 per patient will be paid for those patients in retention. This value is based on 50% of £49 which is the cost per patient to conclusion, based on the costs identified in the patient pathway. See Annex 9.3 for further details;
- Where a patient in active treatment requires a repair of a fixed orthodontic appliance this is accounted for in the close down payment;
- When calculating the close down payments, Commissioners must use these agreed values. It is not appropriate to apply this calculation using local UOA values. A template has been provided in Annex 9.4 accompanying this policy to calculate the value of close down payments;
- Close down arrangements do not apply to Contractors who have been successful in the re-procurement process. In these cases, the Contractor will continue to treat their existing caseload.
9.4.3 Commissioner process for implementing orthodontic close down arrangements
- The Commissioner, on receipt of notice of termination by a Contractor or at time of contract notification during procurement, will begin discussions with the outgoing Contractor to discuss the continuation of clinical care for patients who are in active treatment (fixed appliance only) or in supervised retention;
- If the Contractor is willing to continue to provide this clinical care, the Commissioner will provide the Contractor with a template form to complete, provided in Annex 3, with details of all the patients under their NHS care. The Contractor must complete this form electronically and submit it back to the Commissioner. Instructions to complete the form are provided in the electronic spreadsheet;
- Where the Contractor does not agree to the close down arrangements, the Commissioner will need to seek alternative arrangements for patient care. The funding should follow the patient;
- The Commissioner will also request a list of the patients held by NHSBSA for this Contractor;
- The Contractor will confirm the premises out of which they will be providing clinical care. Where this is not the existing premises the Commissioner will need to confirm their suitability for provision of clinical care and that its location still meets the needs of the patients and the commissioning intentions of the Commissioner. Where the premises are not deemed suitable, the Commissioner may refuse to allow the Contractor to go forward with close down arrangements and will seek alternative arrangements for patient care or the Contractor can make alternative arrangements;
- The Commissioner will reconcile the data sets and will query with the Contractor where there are missing patients (i.e. on NHSBSA list but not Contractor or vice versa) and agree a finalised list with the Contractor;
- Based on the reconciled data set the Commissioner will calculate how many patients are in active treatment (fixed appliance only) or in supervised retention
- The Commissioner will calculate the longest period a patient may remain under the clinical supervision of the Contractor;
- Contractor agrees to provide close down arrangements on basis of number of patients on list and payment OR Contractor does not agree to close down arrangements and the Commissioner need to seek alternative arrangements for patient care.
The Commissioner will agree with the Contractor the payment arrangements. The payment is a one-off payment per patient regardless of length of treatment.
The total payment will be calculated and paid over a minimum period of 12 months, or longer by mutual agreement between the contract and Commissioner.
The agreed payment schedule will form part of the PDS variation notice.
The flow chart describes the process a Commissioner should take when implementing close down arrangements.
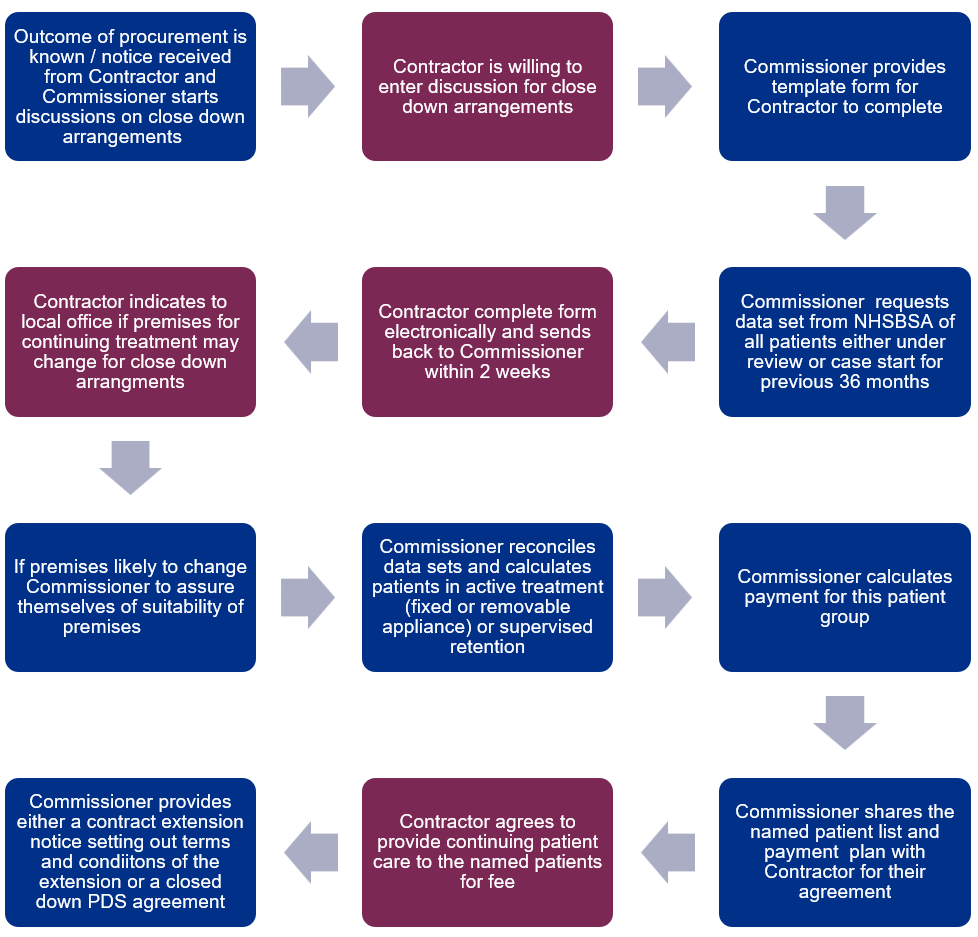
- Where the contract is ending due to a procurement process or it is the end of the natural PDS agreement period, the Commissioner will apply for a single tender action (STA) using NHS England agreed processes for an extension to the PDS agreement for a period not exceeding the length of treatment for the last patient to be completed by the Contractor.
- When the STA has been made, the Commissioner will extend the PDS agreement which will also be varied to remove the contracted UOA levels and associated remuneration and for the new payment arrangements to be implemented. An example PDS variation notice is provided in Annex 5.
- Where the contract is ending due to a procurement process or it is the end of the natural PDS agreement period and the STA extension has ended, the Commissioner will terminate the existing agreement and issue a new PDS agreement specifically for patients in active treatment in order to aid with closedown. The template model contract is available on the NHS England website.
- Where the contract is terminating due to notice by the Contractor but within the timeframe of the current contract, the PDS agreement will be varied to remove the contracted UOA levels and associated remuneration and for the new payment arrangements to be implemented.
- The Commissioner to send documentation to the practice for signature of the Contractor
- The Contractor to sign and return documents.
- The Commissioner to sign documents and send a signed copy to the Contractor.
- The Commissioner to amend Compass noting new end dates, removing UOA level and associated contract payments and adding new payment levels.
- The Contractor provides clinical care to patients in active treatment (fixed appliance only) and in supervised retention.
- The Contractor does not provide any new case assessments or case starts.
- The Contractor submits FP170 to NHSBSA on completion of active treatment / supervised retention.
- The Commissioner monitors activity of contract during period of orthodontic close down.
- Failure by the Contractor to complete the courses of treatment within projected time scales other than for reasons of patient choice, the Commissioner can review the payment received and the Contractor may be liable for repayment of funds received.
- On completion of the PDS extension or new agreement the contract is closed and ended on Compass.
The flow chart describes the process a Commissioner should take when implementing close down arrangements.
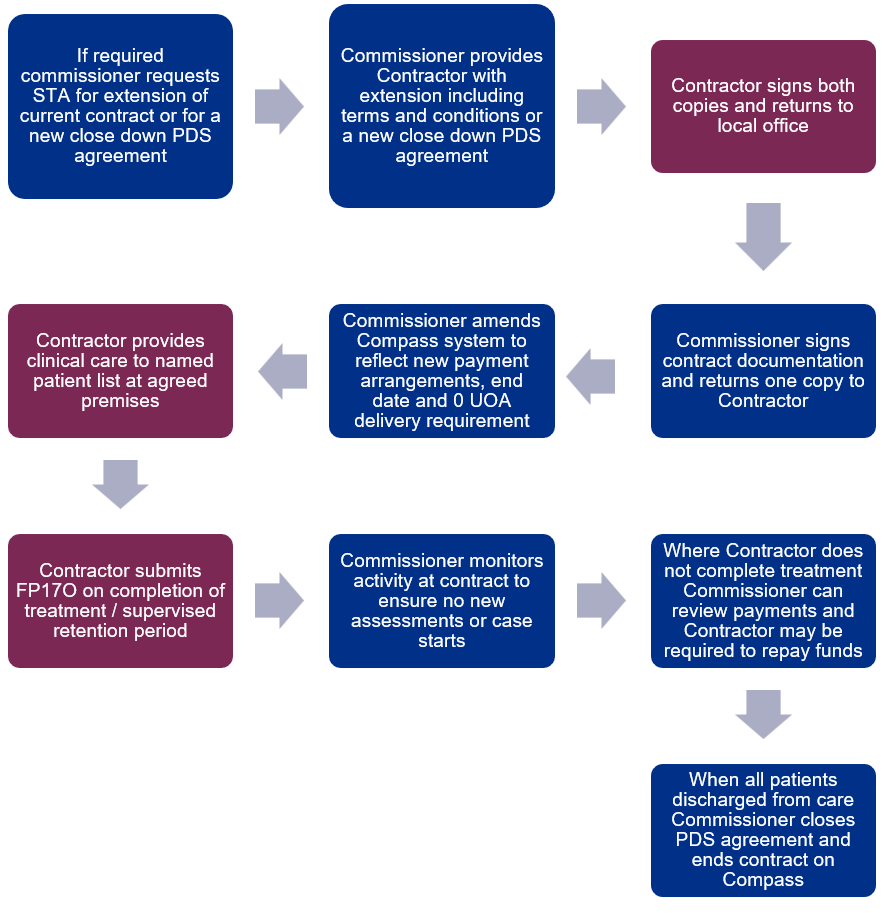
10. Contract breaches
10.1 Introduction
This chapter outlines the approach to be taken when primary dental services contracts are considered to have been breached. Breach notices in regard to non delivery of contractual activity within tolerance is previously covered under section 8.4.4 of this policy book. Where processes differ with regards GDS contracts and PDS agreements, these are highlighted.
Given that any decision to issue a Remedial or Breach Notice, apply contract sanctions or terminate a contract can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Commissioners should maintain accurate records of all breaches and will be required to demonstrate if requested, evidence of compliance, or otherwise support oversight of primary dental care commissioning arrangements.
It is important to keep a clear record of each step along the way – what happened, when, why, who was involved– so that the Commissioner is able to show that they have acted reasonably throughout and in accordance with the relevant regulations.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 10.1: Remedial Notice Flowchart
- Annex 10.2: Template Remedial Notice
- Annex 10.3: Template Remedial Notice Satisfaction Letter
- Annex 10.4: Breach Notice Flowchart
- Annex 10.5: Template Breach Notice
10.2 Contract breaches
Where the Commissioner considers that a breach has occurred, there are several options on how to proceed. The Commissioner can:
- agree an action with the Contractor;
- issue a Remedial Notice;
- issue a Breach Notice;
- apply a contract sanction; or
- terminate the contract.
Agreeing an action with the Contractor is an option that is always available to the Commissioner. The remaining options may only be applied in specific situations as envisaged by the contract. The decision as to which option to take should be made regarding all internal processes, complies with any standing orders and considers all relevant factors.
Commissioners should confirm in writing if they are taking no further action, or provide a written action plan, including required actions and timescales for completion. Any communication with the Contractor should be noted and held on file as this may form part of any evidence of local resolution or for future consideration of contracting matters.
The following paragraphs set out the circumstances in which a Remedial Notice or a Breach Notice may be issued and the process that the Commissioner must follow. See Chapter 11 ‘Contract Terminations and Sanctions’ for further information on these contractual actions.
Where a contract has been breached the Commissioner must decide whether to issue a breach or Remedial Notice.
There are several circumstances where the Commissioner has a right to terminate the contract immediately for a breach:
- provision of untrue information;
- on grounds of suitability;
- a serious risk to patient safety or risk of material financial loss to NHS England; and
- in the case of a GDS contract, issues relating to the Contractor’s eligibility to hold the contract.
In doing so the Commissioner must behave reasonably. These rights of termination are explained in more detail in Chapter 11.
10.3 Remedial notices and breach notices
The GDS and PDS Regulations make a clear distinction between the process to be followed where a breach is capable of remedy and the process where a breach is not capable of remedy.
Where a breach is capable of remedy, a Remedial Notice must be issued before the Commissioner takes any other action under the contract (such as termination). Where a breach is not capable of remedy, a Breach Notice must be issued before the Commissioner takes any other action under the contract (such as termination).
10.3.1 Remedial notice
Where a Contractor has breached the contract and the breach is determined to be capable of remedy the Commissioner may issue a Remedial Notice to the Contractor setting out the actions that must be taken to remedy the breach.
A flowchart highlighting the main steps that the Commissioner should take when issuing a Remedial Notice is set out in Annex 10.1.
A breach capable of remedy is where the breach continues but the Contractor can take action to stop the breach. Examples of breaches that may be capable of remedy include:
- failure to compile a patient information leaflet;
- failure to keep premises clean; or
- failure to provide information to the Commissioner.
Where the breach creates a serious risk to patient safety, the Commissioner has the right to terminate immediately. See Chapter 11 for further information.
Where the Commissioner has determined that a breach is capable of remedy the Commissioner may, depending on the nature and circumstances of a breach take the following steps. These steps do not prejudice or delay a Commissioner’s right to issue a Remedial Notice at any point before or during any of these steps being taken where the Commissioner reasonably considers it is appropriate to do so:
- Initially the Commissioner should contact the Contractor to discuss the breach and the action that they may be entitled to take, i.e. the issue of a Remedial Notice.
- The Contractor should be afforded the opportunity to provide an explanation as to the circumstances that led to the breach and this discussion should be recorded accurately in writing.
- The Commissioner should review the evidence related to the breach including any information received during the discussion or in representations.
- If the Commissioner is satisfied that the matter is a breach which is capable of remedy, then the Commissioner may issue a Remedial Notice to the Contractor, requiring the Contractor to remedy the breach.
- It is important that when the steps above are undertaken, this is completed as quickly as is reasonably possible as long delays between the breach occurring, or the Commissioner becoming aware of the breach, and the Remedial Notice being issued could lead to an argument that the Commissioner has accepted the breach and waived its right to act. The Commissioner will need to decide what action it considers would be reasonable to take before issuing a Remedial Notice considering the circumstances of an individual breach.
- During the initial stages if the Commissioner decides the breach is significant it can issue a Remedial Notice at any point in the process.
10.3.2 The Remedial Notice must specify:
- the clause number(s) and text of the clause(s) that have been breached;
- details of the breach, which led to the Remedial Notice being issued and any evidence gathered in respect of the breach;
- the steps the Contractor must take to remedy the breach to the Commissioner’s satisfaction;
- the period in which the steps must be taken;
- any arrangements for reviewing the matter to ensure that the requirements of the Remedial Notice have been met; and
- the actions that the Commissioner shall take if the Contractor fails to satisfactorily remedy the breach; and
- the dispute rights of the Contractor.
A template Remedial Notice is provided in Annex 10.2. The finalised Remedial Notice should be signed off by off by the appropriate person within the commissioning organisation.
The period during which the steps to remedy the breach must be taken must not be less than 28 days from the date that notice is given, unless the Commissioner is satisfied that a shorter period is necessary to protect the safety of the Contractor’s patients or protect NHS England from material financial loss.
The Remedial Notice must be delivered to the Contractor in accordance with the notice provisions of the contract. This usually requires postal delivery (signed for or registered post). Delivery of a notice by email may be permissible. The Commissioner should review the relevant provisions to the contract to ensure proper delivery.
The Commissioner should ensure that arrangements are in place to follow up a Remedial Notice appropriately and in a timely fashion. A declaration of remedy should be sought from the Contractor to confirm their compliance.
Where the Commissioner is satisfied that the Contractor has taken the required steps to remedy the breach within the required period, a letter should be issued to the Contractor informing them that the terms of the Remedial Notice have been satisfied and that no further action will be taken at this stage, but the breach remains on file. A template Remedial Notice satisfaction letter is provided in Annex 10.3.
Where the Commissioner is satisfied that the Contractor has not taken the required steps to remedy the breach by the end of the required notice period, the Commissioner may inform the Contractor that they have failed to meet the terms of the Remedial Notice and that the Commissioner may issue a contract sanction or terminate the contract with effect from such date as the Commissioner may specify in a further notice to the Contractor.
Where the Commissioner intends to terminate the contract, please refer to the Key Considerations on Termination in Chapter 11.
If, following the issue of a Remedial Notice, a Contractor either repeats a breach that was the subject of a Remedial Notice or otherwise breaches the contract that results in a further Remedial Notice or a Breach Notice, then the Commissioner has the right to terminate the contract by serving notice on the Contractor.
The right to terminate above must only be used where the Commissioner is satisfied that the cumulative effect of the breaches is such that the Commissioner considers that to allow the contract to continue would be prejudicial to the efficiency of the services to be provided under the contract. Where the Commissioner intends to terminate the contract under this right, please refer to Chapter 11 in the section ‘Termination relating to Remedial Notices and Breach Notices’.
If the Contractor is in breach of any obligation and a Remedial Notice in respect of that breach has been given to the Contractor, the Commissioner may withhold or deduct monies which would otherwise be payable under the contract in respect of that obligation which is the subject of the breach.
Where the Contractor disputes the Commissioner’s decision to issue a remedial Breach Notice, the Contractor may invoke the dispute resolution procedure as outlined in their contract. In such circumstances, the Commissioner should follow Chapter 13 ‘Managing Disputes’.
10.3.3 Breach notice
Where the Contractor has breached the contract and that breach is not capable of remedy, the Commissioner may serve a Breach Notice on the Contractor stating what has been breached and requiring the Contractor not to repeat the breach.
A flowchart highlighting the main steps that the Commissioner should take when issuing a Breach Notice is set out in Annex 10.4.
A breach that is not capable of remedy is where a breach occurs but either has stopped prior to a notice being issued or there is no action that can be taken to remedy the breach.
An example of a breach that is not capable of remedy is a practice closing during its contracted opening times with no access for the Contractor’s patients to access mandatory services.
Where the breach creates a serious risk to patient safety, the Commissioner has the right to terminate immediately. See Chapter 11 for further information.
Where the Commissioner has determined that a breach is not capable of remedy, the Commissioner may, depending on the nature and circumstances of a breach take the following steps. These steps do not prejudice or delay a Commissioner’s right to issue a Breach Notice at any point before or during any of these steps being taken where the Commissioner reasonably considers it is appropriate to do so:
- Initially the Commissioner should contact the Contractor to discuss the breach and the action that they may be entitled to take, i.e. the issue of a Breach Notice. This does not prejudice or delay a Commissioner’s right to issue a Breach Notice.
- The Contractor should be afforded the opportunity to provide an explanation as to the circumstances that led to the breach and this discussion should be recorded accurately in writing.
- The Commissioner should review the evidence related to the breach including any information received during the discussion or in representations.
- If the Commissioner is satisfied that the matter is a breach which is not capable of remedy, then the Commissioner may issue a Breach Notice to the Contractor, requiring the Contractor not to repeat the breach.
- During the initial stages if the Commissioner decides the breach is significant it can issue a Breach Notice at any point in the process.
10.3.4 The Breach Notice must specify:
- the clause number(s) and text of the clause(s) that have been breached;
- details of the breach(es), which led to the Breach Notice being issued and evidence gathered in respect of the breach(es);
- the requirement that the Contractor must not repeat the breach again;
- the consequences of the Contractor further breaching their agreement; and
- the dispute rights of the Contractor.
A template Breach Notice is provided in Annex 10.5. The finalised Breach Notice should be signed off by the appropriate person within the commissioning organisation.
The Breach Notice must be delivered to the Contractor in accordance with the notice provisions of the contract as described within section 10.3.2.
If, following the issue of a Breach Notice, a Contractor either repeats a breach that was the subject of a Breach Notice or otherwise breaches the contract that results in a further Remedial Notice or a Breach Notice, then the Commissioner has the right to terminate the contract by serving notice on the Contractor.
This right to terminate can only be used where the Commissioner is satisfied that the cumulative effect of the breaches is such that the Commissioner considers that to allow the contract to continue would be prejudicial to the efficiency of the services to be provided under the contract. Where the Commissioner intends to terminate the contract under this right, please refer to Chapter 11 in the section ‘Termination relating to Remedial Notices and Breach Notices’.
If either of the following circumstances occurs and the time in the relevant circumstances has elapsed, the Commissioner shall act as if the Breach Notice was not issued. The Commissioner will not look to rely on the Breach Notice when taking any future actions under the GDS contract or PDS agreement:
- A Breach Notice is issued to a Contractor who has achieved between 90% and less than 96% of a contract’s UDA/UOA target in a particular financial year and, in the following two financial years, the Contractor achieves 96% or more of the contract’s UDA/UOA target.
- A Breach Notice is issued to a Contractor who has under-delivered against the contract’s UDA/UOA target in a particular financial year and, in a following year, the Contractor and Commissioner agree a recurrent rebase of the contract’s UDA/UOA target.
If the Contractor is in breach of any obligation and a Breach Notice has been issued the Commissioner may withhold or deduct monies which would otherwise be payable under the contract in respect of that obligation.
Where the Contractor disputes the Commissioner’s decision to issue a Breach Notice, the Contractor may invoke the dispute resolution procedure as outlined in their contract. In such circumstances, the Commissioner should refer to Chapter 13 ‘Managing Disputes’.
11. Contract terminations and sanctions
11.1 Introduction
This chapter outlines the approach when a decision has been taken to apply a contract sanction or terminate a contract.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 11.1: Calculating a financial contract sanction
- Annex 11.2: Template contract sanction notice
- Annex 11.3: Template termination notice
- Annex 11.4: Termination flowchart
- Annex 11.5: Extract from GDS contract – suitability
- Annex 11.6: Extract from PDS agreement – suitability
11.2 Contract sanctions
Contract sanctions must not be applied to a contract unless the Commissioner is in a position to move to terminate. Where contract sanctions are applied, this is as an alternative to terminating the contract. The Commissioner cannot apply contract sanctions and later decide to terminate the contract for the same circumstances.
Where a decision has been made to apply contract sanctions the Commissioner must follow the process set out in this section.
PDS agreements refer to “agreement sanctions” rather than contract sanctions. Reference to contract sanctions in this section should be read as including reference to agreement sanctions.
The circumstances in which the Commissioner may apply contract sanctions are set out below where a right of termination arises. Please refer to the relevant right of termination for further information on how these rights of termination arise:
- provision of untrue information;
- on grounds of suitability;
- where there is a serious risk to patient safety or NHS England is at risk of material financial loss;
- where the Commissioner is satisfied that the Contractor has not taken the steps required by a Remedial Notice to remedy a breach within the required period;
- where, after a Remedial Notice or Breach Notice has been issued, the Contractor:
- repeats a breach that was the subject of a Remedial Notice or a Breach Notice; or
- otherwise breaches the contract resulting in a further Remedial Notice or Breach Notice;
- where the Contractor carries on business detrimental to the contract;
- where the Contractor is a dental corporation (and for PDS agreements, a company limited by shares) and there are certain matters relating to the directors of the dental corporation (or the company limited by shares), and Article 39 of the Dentists Act Order comes fully into force;
- for GDS contracts, where changes in the membership of the partnership (or a limited liability partnership) is likely to have a serious adverse impact on the ability of the Contractor or the Commissioner to perform obligations under the contract;
- for PDS agreements, where:
- the Contractor is a company limited by shares and the company ceases to be a company limited by shares or fails to satisfy certain conditions;
- the Contractor is a limited liability partnership, and the partnership ceases to be a limited liability partnership or fails to satisfy certain conditions.
Contract sanctions must not be applied if they terminate or suspend any obligation that relates to mandatory services.
Contract sanctions may involve:
- termination of specified reciprocal obligations;
- suspension of specified reciprocal obligations for a period of up to six months; or
- withholding or deducting monies otherwise payable under the contract.
The choice of which contract sanction to use would ordinarily depend on the nature of the right to terminate, and what is felt to be the most reasonable, appropriate, and proportionate action in those circumstances.
Where the Commissioner decides that the most appropriate sanction would be to withhold or deduct monies, this must be calculated in accordance with set criteria in order to establish a consistent, fair, and measured approach. Annex 11.1 provides further information on calculating a financial contract sanction.
Where the Commissioner decides to impose a contract sanction, the Commissioner must issue a notice of its intent to apply a sanction to the Contractor which must include:
- the nature of the sanction to be applied;
- if withholding or deducting monies, how this has been calculated and the duration of any such sanction;
- if services are to be terminated, which services and from what date;
- if suspension of specified reciprocal obligations under the contract or agreement, the period of that suspension and its end date;
- an explanation of the effect of the imposition of the contract sanction; and
- the dispute rights of the Contractor
A template contract sanction notice is provided in Annex 11.2. The finalised contract sanction notice should be signed off by the appropriate person in the commissioning organisation.
The date that the contract sanction takes effect must not be until at least 28 days after the notice was served unless the Commissioner is satisfied that it is necessary to impose the contract sanction to protect the safety of patients or protect the NHS from material financial loss.
Where a contract sanction is imposed, the Commissioner can charge the Contractor reasonable administration costs of imposing the contract sanction.
If the Contractor disputes the imposition of a contract sanction, the Commissioner must not impose the contract sanction until the dispute has been determined unless the contract sanction is necessary to protect the safety of patients or protect the NHS from material financial loss.
Where a dispute arises in relation to the imposition of a contract sanction, please refer to Chapter 13 ‘Managing Disputes’.
The Commissioner should ensure that arrangements are in place to monitor the Contractor’s compliance with a contract sanction notice.
11.3 Termination
The GDS and PDS Regulations set out certain rights of termination that are required to be in the different types of primary dental contract. These mandatory termination rights are set out below. Where the termination relates to a matter that is contained within an alternative policy, this is highlighted.
Termination is a very significant action to take both on the part of the Commissioner and the Contractor and is an area of high risk for both parties in respect of financial impact and continuity of services. It is essential that the Commissioner maintains thorough and accurate records of all communications and discussions in respect of all notices.
Contractors have the right to appeal so it is essential that the Commissioner follows and can demonstrate that they have followed due process in investigating, communicating and implementing actions leading to termination.
It is essential that prior to moving to terminate a contract, the Commissioner is satisfied that they are fully within their rights to do so.
The contract may contain additional termination rights. The Commissioner should consider the relevant contract to ensure it is fully aware of all termination rights.
The following circumstances relating to rights of termination are required to be in GDS contracts and PDS agreements:
- agreement of the parties;
- death of a Contractor;
- Contractor serving notice;
- late payment;
- provision of untrue information;
- suitability;
- patient safety;
- material financial loss;
- Remedial Notices and Breach Notices;
- carrying on business detrimental to the contract; and
- certain matters relating to directors of dental corporations.
GDS contracts are required to contain additional rights of termination relating to:
- no longer eligible to enter into and breach of conditions of the contract;
- certain matters relating to the ceasing of a limited liability partnership; and
- certain partnership (including limited liability partnership) matters.
PDS agreements are required to contain additional rights of termination relating to:
- certain matters relating to directors of a company limited by shares;
- certain matters relating to the ceasing of a company limited by shares and/or a limited liability partnership; and
- Contractor’s exercise of the right to a GDS contract.
Contracts may also terminate or expire by:
- reaching their natural end dates (in which case, please refer to Chapter 15 – ‘Practice Closedowns’ for more information);
- contract novation (in which case, please refer to the policy on contract variations); and
- Retirement of the Contractor (in which case, please refer to the policy on contract variations).
Where the Commissioner has considered all the relevant factors and has decided to proceed with termination, it must send a termination notice to the Contractor.
The termination notice must specify:
- the clause number(s) and text of the clause(s) that have been breached which give rise to the right to terminate
- the reason for the right to terminate
- the dispute rights of the Contractor
A template termination notice is provided in Annex 11.3. The finalised termination notice should be signed off by the off by the appropriate person within the commissioning organisation.
Where the termination relates to:
- for GDS contracts and PDS agreements:
- provision of untrue information;
- suitability;
- patient safety;
- material financial loss;
- Remedial Notices and Breach Notices;
- carrying on business detrimental to the contract; and
- certain matters relating to directors of dental corporations
- for GDS contracts:
- certain matters relating to the ceasing of a limited liability partnership; and
- certain partnership (including limited liability partnership) matters,
- for PDS agreements:
- certain matters relating to directors of a company limited by shares; and
- certain matters relating to the ceasing of a company limited by shares and/or a limited liability partnership.
The notice must specify a date on which the contract terminates that is not less than 28 days after the date on which the Commissioner has served the notice on the Contractor. The Commissioner may state a date less than 28 days where this is necessary to protect the safety of the Contractor’s patients or protect the Commissioner from material financial loss.
Where the Contractor disputes the Commissioner’s decision to terminate the contract, the Contractor may invoke the NHS dispute resolution procedure. In such circumstances, the Commissioner should refer Chapter 13 – ‘Managing Disputes’.
11.4 Key considerations on termination
The Commissioner must establish that grounds exist under the terms of the contract to terminate. The Commissioner must follow due process and investigation of the facts and provide the contactor with the opportunity to provide a response to allegations, wherever possible.
Initially the Commissioner should contact the Contractor to discuss grounds under which they may take contractual action i.e. termination
- the Contractor should be afforded the opportunity to provide an explanation as to the circumstances and this discussion should be recorded accurately in writing.
- the Commissioner should then investigate the grounds for termination, including any details recorded during the Contractor discussion which are pertinent to the matter and examine any evidence.
- if the Commissioner is satisfied that there are grounds to terminate then a termination notice must be sent.
There may be occasions where it is not appropriate to initially contact the Contractor about the issues under investigation and this will be decided on a case-by-case basis.
A flowchart highlighting the main steps that the Commissioner should take when issuing a termination notice is set out in Annex 11.5.
The Commissioner must consider all relevant information available and decide on the appropriate course of action and whether the contract should be terminated.
Apart from considerations regarding whether the right to terminate arises, there are a few factors that the Commissioner should consider when termination is a proposed course of action. These factors are set out below.
This list is not exhaustive and there are likely to be other issues that need due consideration under these provisions. These considerations will also apply following the sudden death of a Contractor, covered in Chapter 12.
11.4.1 Continuity of service provision
NHS England has a statutory duty to ensure continuity of provision of primary care services. Termination of existing service provision may result in some persons not being able to access primary dental services. The Commissioner must therefore consider how this duty will be discharged if it decides to terminate the contract.
If the Commissioner envisages that a new contract will be entered into with a provider, the Commissioner must consider how to procure that contract and to ensure it is in accordance with procurement law and any procurement protocol issued by NHS England.
The Commissioner should ensure that it is able to signpost any patients seeking treatment, to other local dentists accepting NHS patients. This may be through making information available at the practice or via NHS 111 services, whichever is relevant.
Where a Termination Notice has been issued, the Contractor should use best endeavours to ensure the completion of all open courses of treatment. This will not be possible where the termination is effective immediately and the Commissioner will need to work with other local dental providers to secure completion of the active courses of treatment.
Patients seeking recourse under free repair and replacement provisions need to be made aware that there will be a fee to pay if a repair and/or replacement treatment is performed by an alternative practice. Similarly, where a continuation of treatment at the same or lower band within two months is needed, patients will be required to pay the relevant dental charge when this is carried out by another provider.
Where a patient is undergoing an orthodontic course of treatment, it is unlikely due to the nature of treatment patterns and their longevity, that treatment can be completed within the Termination Notice period. The Commissioner should work with the Contractor’s representatives to:
- obtain copies of any orthodontic health records for patients currently in treatment that could then be provided to an alternative provider; and
- obtain patients’ details so they can be contacted regarding continuation of their treatment.
The Commissioner will need to secure alternative provision for those patients undergoing a course of orthodontic treatment. This can be with other local orthodontic providers, or they may need to consider commissioning these services from secondary care providers where alternative primary orthodontic care provision is not available.
Currently the GDS contract or PDS agreement and the relevant SFE state the level of payment for an orthodontic course of treatment. Due to the payment structure and length of an orthodontic course of treatment, the Commissioner may wish to raise the cost pressures of paying for these patient transfers within its risk register. Payments should be made in accordance with the section on orthodontic close down arrangements set out in Chapter 9.
The Commissioner may wish to procure additional activity from orthodontic providers on a non-recurrent basis, on a case-by-case fee structure while they consider whether procure a contract or agreement. If this is the path that is chosen by the Commissioner, it would be advisable to access specialist procurement and legal advice.
11.4.2 General duties of NHS England
Under section 13 of the NHS Act, NHS England has several statutory duties relating to the exercise of its functions including reducing health inequalities and patient involvement. The Commissioner must ensure that its actions in terminating a contract and any consequential actions ensure compliance with the section 13 duties and other applicable statutory duties of NHS England. In an urgent situation, it may be necessary to balance the duty to involve patients with the public interest in maintaining continuity of care and protecting the health, safety and welfare of patients or staff. Please refer to Chapter 2 ‘General Duties of NHS England’ for more information on the scope of the duties.
NHS England has set out its plans as to how it intends to involve the public in the following publications:
- The Patient and Public Participation Policy
- The Statement of Arrangements and Guidance on Patient and Public Participation in Commissioning.
- The Framework for Patient and Public Participation in Primary Care Commissioning.
11.4.3 Premises
The Commissioner should ascertain who owns the premises and what arrangements apply to the premises. Where the outgoing Contractor controls the premises, a future service provider may not be able to use those premises for delivery of services. The Commissioner should consider what arrangements need to be put in place to ensure continued service provision.
11.4.4 Transfer of Undertakings (TUPE)
The Commissioner should consider the impact of termination on the staff currently employed under the terminating contract. Where a new contract is entered into with a new provider, TUPE may apply to transfer the staff to the new provider.
TUPE can be complex, high risk and time consuming for any incoming provider and is likely to have a financial impact on the cost of any service. The Commissioner should consider whether the potential for TUPE to apply may be considered a significant risk to any incoming provider.
11.4.5 Equipment
Some equipment may be owned by the Commissioner. Arrangements may need to be put in place to retrieve this equipment to ensure it is available to a future service provider.
11.4.6 Patient records
Where it is not possible to complete patients’ treatments within the termination notice period, arrangements must be made to transfer patient records securely to any other local dental providers that are completing the courses of treatment. Patients should be fairly notified of the transfer.
11.4.7 Prescriptions
The Commissioner should consider prescription pads, electronic prescriptions, and any uncollected completed prescriptions – these will also need to be retrieved and dealt with accordingly. The Commissioner may wish to decide on a specified age of a current prescription (such as one month) and make appropriate arrangements for the handling of these and disposal of any that are older.
11.4.8 Drugs and medicines
The Commissioner should consider practice held drugs – these will need to be disposed of but are technically likely to be owned by the Contractor whose contract is terminating. The Commissioner should seek assurances about the safe and effective disposal of such drugs.
11.4.9 Financial Reconciliation
On termination of a GDS contract or PDS agreement, the Commissioner will need to carry out a financial reconciliation in line with the relevant SFE. For further information on this, please refer to Chapter 8 ‘Financial Recovery and Reconciliation’.
11.5 Rights of Termination
Given the serious nature of termination irrespective of who instigates it, it is essential that the Commissioner follows, and can demonstrate that it has followed, due process in investigating, communicating and implementing actions in this respect and that the Commissioner has acted fairly and reasonably throughout.
Commissioners should maintain accurate records of all activities in respect of the termination process and will be required to demonstrate if requested, evidence of compliance, or otherwise support oversight of primary dental care commissioning arrangements.
It is important to keep a clear record of each step along the way – what happened, when, why, who was involved – so that the Commissioner is able to show that they have acted reasonably throughout and in accordance with the relevant regulations.
Under section 13 of the NHS Act, NHS England has several statutory duties relating to the exercise of its functions including reducing health inequalities and patient involvement. The Commissioner must ensure that its actions in terminating a contract and any consequential actions ensure compliance with the section 13 duties and other applicable statutory duties of NHS England. In an urgent situation, it may be necessary to balance the duty to involve patients with the public interest in maintaining continuity of care and protecting the health, safety and welfare of patients or staff. Please refer to the Chapter 2 ‘General Duties of NHS England’ for more information on the scope of the duties. All circumstances set out in section 12.6 below would need to consider if the general duties of NHS England are triggered.
11.6 Termination circumstances
11.6.1 Termination where both parties agree
Where the parties agree to terminate, the parties must agree the date from which termination will take place and any further terms relating to the termination. Before agreeing the termination date, the Commissioner should ensure any proposed timescale allows the Commissioner to consider any other factors or actions that may be required prior to termination.
The Contractor party may comprise of more than one person. The Commissioner must agree the same termination arrangements with all persons that constitute the Contractor.
11.6.2 Termination where the Contractor serves notice
Contracts can be terminated by the Contractor by serving notice in writing at any time.
Where a Contractor serves notice to terminate, it shall terminate three months after the date on which the notice is served.
If the date on which the contract will terminate is not the last calendar day of a month, the contract shall instead terminate on the last calendar day of the month in which the termination date falls. For example, if the termination date is the 16 of April, then the contract will terminate on the 30 of April in the specified year.
Please refer to section 15.11 Management of Contract Hand backs for further information.
11.6.3 Termination where the Contractor exercises the right to a GDS contract
Please refer to Chapter 7 ‘Managing a PDS Contractor’s Right to a GDS
Contract’ for further information.
11.6.4 Termination due to late payment
The Contractor may give notice in writing to the Commissioner if the Commissioner has failed to make any payment due to the Contractor under the contract. If the Commissioner has failed to make any such payment within 28 days of the notice, the Contractor may terminate the contract by a further written notice.
Where the NHS dispute resolution procedure has been invoked by the Commissioner, the Contractor may not terminate the contract until either the NHS dispute resolution determination allows termination, or the Commissioner ceases to pursue the NHS dispute resolution process. Any such dispute resolution process must be commenced within 28 days of the initial notice received from the Contractor.
For further information on the NHS dispute resolution process, please refer to Chapter 13 ‘Managing Disputes’.
11.6.5 Termination for provision of untrue information
The Commissioner may serve notice to terminate the contract immediately (or from any date set out in the notice) if, after the contract has been entered into, it comes to the attention of the Commissioner that written information provided to the Commissioner:
- before the contract was entered into; or
- for GDS contracts, pursuant to paragraph 42(2) of Schedule 3 of the GDS Regulations, in relation to regulations 4 and 5 of the GDS or PDS Regulations (whichever is applicable) was, when given, untrue or inaccurate in a material respect.
11.6.6 Termination due to suitability
The Commissioner may serve notice in writing on the Contractor terminating the contract immediately (or from any date set out in the notice) where a person connected with the contract (such as a dental practitioner, a partnership, a limited liability partnership, a dental corporation, a company, or a director) falls within any circumstances set out in the relevant regulations. Those circumstances include where the person:
- has been disqualified, removed from, or refused admittance on to various licensing bodies;
- has been convicted of certain offences;
- has been adjudged bankrupt; or
- has been subject to a disqualification under the Company Director Disqualification Act 1986.
Details of the type of person connected with the contract and a full list of the relevant circumstances is set out in Annex 11.6 for GDS contracts and Annex 11.7 for PDS agreements.
11.6.7 Termination where there is a serious risk of patient safety
The Commissioner may serve notice in writing on the Contractor terminating the contract immediately (or from such date set out in the notice) where the Contractor has breached the contract and, because of that breach, the safety of the Contractor’s patients is at serious risk if the contract is not terminated.
11.6.8 Termination where there is a risk of material financial loss to NHS England or ICB
The Commissioner may serve notice in writing on the Contractor terminating the contract immediately (or from such date set out in the notice) where the Contractor’s financial situation is such that the Commissioner considers that there is a risk of material financial loss.
11.6.9 Termination relating to Remedial Notices and Breach Notices
The Commissioner has a right to terminate the contract where the Commissioner is satisfied that the Contractor has not taken the required steps to remedy the breach by the end of the required period as stated in the Remedial Notice.
The Commissioner has a further right of termination where, following the issue of a Remedial Notice or Breach Notice, a Contractor:
- repeats a breach that was the subject of a Remedial Notice or Breach Notice; or
- otherwise breaches the contract that results in a further Remedial Notice or Breach Notice.
The further breach must have occurred after the breach which was the subject of the Remedial Notice or Breach Notice. The Commissioner may intend to issue a further Remedial Notice or Breach Notice for a breach that occurred prior to the original breach with the need to investigate or gather information delaying the issue of the notice. In these circumstances, the Commissioner cannot then rely on this right of termination as the further breach did not occur following the issue of the original Remedial Notice or Breach Notice.
This further right to terminate can only be used where the Commissioner is satisfied that the cumulative effect of the breaches is such that the Commissioner considers that to allow the contract to continue would be prejudicial to the efficiency of the services to be provided under the contract. The Commissioner should ensure that it is not looking to rely on a previous Breach Notice in the circumstances set in Chapter 10.
11.6.10 Termination due to the Contractor carrying on business detrimental to the contract
Where the Contractor is:
- a dental corporation under a GDS contract; or
- a dental corporation, a company limited by shares or a limited liability partnership under a PDS agreement, that is carrying on business which the Commissioner considers is detrimental to the performance of the contract, the Commissioner may give notice to the Contractor requiring that it ceases carrying on the relevant business within a specified period which must not be less than 28 days from the date the notice was given.
Where the Contractor has not satisfied the Commissioner that it has ceased carrying on the business by the end of the notice period, the Commissioner may by further written notice terminate the contract immediately (or from such date set out in the notice).
11.6.11 Termination due to certain matters relating to directors of dental corporations
If a Contractor is a dental corporation under a GDS contract or PDS agreement, there are certain matters which allow the Commissioner to issue a Termination Notice provided that those matters lead to the Commissioner considering that the dental corporation is no longer suitable to be a Contractor.
The three matters are:
- if the majority of the directors of the dental corporation cease to be either dental practitioners or dental care professionals,;
- the dental corporation has been convicted of an offence under section 43(1) of the Dentists Act 1984; or
- the dental corporation, or a director or former director of that corporation, has had a financial penalty imposed on it or him by the General Dental Council pursuant to section 43B or 44 of the Dentists Act 1984.
11.6.12 Certain matters relating to directors of a company limited by shares
Under a PDS agreement, the section above, entitled Termination due to certain matters relating to directors of dental corporations also applies where the Contractor is a company limited by shares and references in those paragraphs to the dental corporation should be read as references to the company limited by shares.
11.6.13 Termination due to partnership (including limited liability partnership) matters
The Commissioner has a right to terminate a GDS contract where:
- the Contractor is two or more persons practising in partnership and one or more partners have left the practice during the contract, and
- the Commissioner reasonably considers that the changes in membership of the partnership is likely to have a serious adverse impact on the ability of the Contractor or the Commissioner to perform its obligations under the contract.
The same right of termination exists where the Contractor under a GDS contract is a limited liability partnership and references to partners should be read as references to members.
Where these circumstances occur, the Commissioner may terminate the contract by notice in writing on such date as is set out in the notice. The notice must contain the Commissioner’s reasons for considering that the change in the membership is likely to have a serious adverse impact on the ability of the Contractor or the Commissioner to perform its obligations under the contract.
The Commissioners should note that this right of termination does not exist where the Contractor is a limited liability partnership under a PDS agreement.
11.6.14 Termination due to certain matters relating to the ceasing of a limited liability partnership
The Commissioner must terminate a GDS contract with a limited liability partnership where the Contractor ceases to be a limited liability partnership or where the Contractor ceases to satisfy the conditions in section 102(2A) of the NHS Act.
Section 102(2A) sets conditions which must be satisfied for a contract to be held and continued to be held by a limited liability partnership. Once condition is that at least one member of the limited liability partnership must be a dental practitioner. There is a further condition relating to who has the power to conduct the partnership’s affairs – either paragraph 7.29.1 or 7.29.2 must be satisfied:
- A member who is a dental practitioner or in the list set out in paragraph 7.29.3 below must have the power to secure that the partnership’s affairs are conducted in accordance with that member’s wishes; or
- If, in any combination of partners or members who, acting together, have the power (or who, if they were to act together, would have the power) to secure that the partnership’s affairs are conducted in accordance with their wishes, at least one of them must be a dental practitioner or in the list set out below.
This list includes:
- an NHS employee,
- an individual who, in connection with the provision of services in accordance with either:
- Article 15B of the Health and Personal Social Services (Northern Ireland) Order 1972; or sections 17C, 50, 64, 92 or 107of the NHS Act;
- is employed by a person providing or performing those services
- a health care professional who is engaged in the provision of services under the NHS Act or the NHS (Wales) Act 2006, or
- an individual falling within section 108(1)(d) of the NHS Act.
The requirement for the Commissioner to terminate also applies where the Contractor is a limited liability partnership and ceases to be so under a PDS agreement. The conditions in section 102(2A) of the NHS Act do not apply to PDS agreements. Instead, the Commissioner must terminate if the Contractor is a limited liability partnership and either the limited liability partnership ceases or section 108(1B) and (1C) of the NHS Act cease to apply to the limited liability partnership. These sections relate to who has the power to conduct the partnership’s affairs.
11.6.15 Termination due to certain matters relating to where the ceasing of a company limited by shares
The Commissioner must terminate a PDS agreement with a company limited by shares where the Contractor ceases to be a company limited by shares or where the Contractor ceases to satisfy the conditions in section 108(1A) of the NHS Act.
Section 108(1A) of the NHS Act relates to conditions for those holding shares in such a company. There are two conditions, both of which must be satisfied:
- every person who owns a share in the company must own it both legally and beneficially, and
- it must not be possible for two or more members of the company who are not persons who fall within Section 108(1)(a) to (e) to hold the majority of the voting rights conferred by shares in the company on any matter on which members have such rights.
11.6.16 Termination due to the Contractor no longer being eligible to enter into and breach of conditions of the contract
The Commissioner must terminate a GDS contract immediately where a contract was entered into with a dental practitioner and the Contractor is no longer a dental practitioner.
However, this requirement to terminate will not apply if the Contractor has been suspended as set out in Regulation 69(6) of the PDS Regulations unless:
- the Contractor cannot satisfy the Commissioner that adequate arrangements for providing services are in place for the suspension period; or
- the Commissioner is satisfied that the contract should be terminated forthwith due to a serious risk to patient safety or due to a risk of material financial loss to NHS England.
The Commissioner must terminate a GDS contract immediately or take the action where the contract is with two or more persons practising in partnership and the requirement that at least one partner is a dental practitioner is no longer satisfied. The requirement to terminate does not apply where this situation occurs due to the death of one of the persons in the partnership. Please refer to Chapter 12 ‘Death of a Contractor’ for further information on the process to follow.
The Commissioner must terminate a GDS contract immediately where the contract was entered into with a dental corporation and the Contractor ceases to be a dental corporation.
11.7 Consequences of termination
Contracts usually contain certain obligations on both parties on termination of the contract. The GDS and PDS Regulations do not set out any requirements for primary dental contracts to contain such provision, but the standard GDS contract contains a number of obligations including provisions relating to:
- co-operation in dealing with any outstanding matters;
- delivering up property owned by the other party; and
- carrying out a financial reconciliation for further information on this, please refer to the policy on financial recovery and reconciliation
The Commissioner should consider the relevant contract to determine what obligations relate to termination.
12. Death of a Contractor
12.1 Introduction
The aim of this chapter is to provide consistency when dealing with the death of a Contractor, whether they are an individual Contractor, in a partnership or a corporate organisation. It includes consideration of GDS contracts and PDS agreements.
This chapter outlines the procedure to follow when the death of a Contractor occurs. This is a rare occurrence, but there are certain steps to follow within agreed timescales that are laid down in legislation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 12.1: Template acknowledgement letter – notification of death
- Annex 12.2: Template acknowledgement letter – continuation of contract
- Annex 12.3: Template acknowledgement letter – continuation of contract after death (partnership)
- Annex 12.4: Template acknowledgement letter – continuation of contract after death (partnership two or more individuals)
12.2 Individual – GDS and PDS Contracts
Where a contract is with an individual dental Contractor and that Contractor dies, the contract must terminate at the end of the period of 28 days after the date of the Contractor’s death unless, before the end of that period:
- the Commissioner has agreed in writing with the Contractor’s personal representatives that the contract should continue for a further period, not exceeding six months after the end of the period of 28 days; and
- the Contractor’s personal representatives have confirmed in writing to the Commissioner that they are employing or engaging one or more dental practitioners to assist in the provision of dental services under the contract throughout the period for which it continues.
Where the Contractor’s personal representatives have confirmed in writing to the Commissioner that they are employing or engaging one or more dental practitioners, the Commissioner should issue a Notification Letter setting out the timescales of the continuation. A template Notification Letter is provided in Annex 12.1.
Where the Commissioner is of the opinion that another Contractor may wish to enter into a contract in respect of the mandatory services which were provided by the deceased dental Contractor then the six-month period may be extended by a period not exceeding a further six months (a maximum of 12 months). A template Notification Letter is provided in Annex 12.2.
The Dentist Act 1984 states at section 41(4) that on the death of a registered dentist who was carrying on a dentist business, that person’s personal representatives; widow, children (or trustees on behalf of his widow or any of his children) may carry on the business for three years after that person’s death. It should be noted that this does not confer the right to an NHS dental contract for the same period.
At 12 months this contract MUST terminate, and during this period the Commissioner needs decide on what will happen with the activity associated with the contract, for example procure, re-commission or not. These decisions will be made in line with local needs assessment and strategic planning information.
12.3 Partnership – GDS Contract
The GDS Regulations state that where the contract is with two or more individuals practising in partnership, the contract shall be treated as made with the partnership as it is from time to time constituted.
The default position in partnership law is that every partnership is dissolved as regards all the partners by the death of any partner. The partners can, however, change this position and agree between themselves that the partnership will not dissolve on the death of any partner. It is likely that most partnerships will have dealt with this issue in their partnership deeds to avoid termination of their contract.
The GDS Regulations require GDS contracts to contain specific provisions relating to the dissolution or termination of partnerships.
Where a partner dies, the GDS Regulations distinguish between GDS contracts that are entered into with a Contractor that consists of only two individuals practising in partnership and those GDS contracts where the Contractor consists of more than two individuals.
12.3.1 Two individuals practising in partnership – GDS Contract
Where the Contractor consists of two individuals practising in partnership and the partnership is dissolved or terminated due to the death of one of the partners, the surviving partner must notify the Commissioner in writing as soon as is reasonably practicable of the death of their partner.
Where the Commissioner receives such a notice, it must acknowledge receipt of the notice in writing.
If the surviving partner is a dental practitioner, the contract will continue with that individual. The Commissioner may vary the contract but only to the extent that it is satisfied it is necessary to reflect the change in status of the Contractor from a partnership to an individual dental practitioner. The Commissioner must notify the Contractor in writing of the wording of the proposed variation and the date upon which that variation is to take effect.
A template Notification Letter is provided in Annex 12.3. A variation agreement will need to be included with this letter. A generic contract variation available in Annex 4.3 can be used and adapted for this purpose. The family representative of the deceased partner does not need to sign the variation documentation.
To provide assurance that the individual is able to meet the contractual obligations, the Commissioner should discuss with the individual continued service delivery options bearing in mind the range of services provided and any potential capacity issues.
If the surviving partner is not a general dental practitioner, the Commissioner will need to terminate the contract. Please refer to Chapter 11 ‘Contract Terminations and Sanctions’ for more information.
12.3.2 More than two individuals practising in partnership – GDS contract
Where there are more than two individuals practising in partnership, the death of one of the partners may result in the partnership being dissolved. This may not always be the case as the partnership arrangements between the partners may state that the partnership will continue or make other provision on the death of a partner that does not result in the dissolution of the partnership.
Where the partnership is not dissolved or terminated, the contract will continue, and the provisions below will not apply provided that the partnership remains eligible to hold a GDS contract. Please refer to eligibility requirements in Chapter 3 ‘Which dental contract when?’.
Where the partnership is dissolved or terminated for whatever reason (which may be due to the death of a partner) and the Contractor consists of more than two individuals practising in partnership, it is possible for the contract to continue with one of the former partners if the following conditions apply:
- the former partner must be nominated by the Contractor, (this does not need the agreement of the deceased family / estate); and
- the former partner must be a dental practitioner.
The nomination of the former partner by the Contractor must be:
- in writing and signed by all the persons who are practising in partnership;
- specify the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner;
- be provided to the Commissioner at least 28 days in advance of the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner; and
- specify the name of the individual dental practitioner with whom the contract will continue, which must be one of the partners.
Where the Commissioner receives such a nomination, it must acknowledge receipt of the notice in writing before the date specified in the nomination as the date on which the Contractor proposes to change its status from that of a partnership to that of an individual dental practitioner. The Commissioner should ascertain on a case-by-case basis which persons are required to sign the nomination.
The Commissioner may vary the contract but only to the extent that it is satisfied it is necessary to reflect the change the status of the Contractor from a partnership to an individual dental practitioner. The Commissioner must notify the Contractor in writing of the wording of the proposed variation and the date upon which that variation is to take effect.
A template acknowledgement letter is provided in Annex 12.4. A variation agreement will need to be included with this letter. A generic contract variation available in Annex 4.3 can be used and adapted for this purpose. The family representative of the deceased partner does not need to sign the variation documentation.
12.4 Two or More Signatories – PDS Agreement
The PDS Regulations do not allow PDS agreements to be treated as made with a partnership. Where individuals are practising in partnership, the PDS agreement will be entered into everyone (who may or may not be in partnership). The individual signatories to a PDS agreement collectively form the Contractor. The PDS Regulations do not require a PDS agreement to define a specific process for any variation to the signatories. The Commissioner must, therefore, review the relevant PDS agreement to determine whether any provisions have been added relating to this and prior to following any process for variation.
A surviving signatory to a PDS agreement will notify the Commissioner in writing as soon as reasonably practicable of the death of their co-signatory.
Upon receipt of the notification from the surviving co-signatory(ies), the Commissioner will need to consider the implications that the death of the co-signatory will have on the ongoing provision of services under the agreement.
Where the Commissioner is satisfied that the remaining signatory (ies) is eligible to hold the agreement and agrees that the agreement is to continue, the agreement will need to be varied to remove the deceased as a signatory.
The process above does not affect any right that the Commissioner may have to terminate the agreement under any terms of the agreement.
12.5 Dental Corporation, Company Limited by Shares and Limited Liability Partnership
Where a contract is entered into with a dental corporation, a company limited by shares or a Limited Liability Partnership, it is not possible for the Contractor to die. It is possible that such Contractors may indicate to the Commissioner where a performer, a member, a director, a chief executive, or a company secretary has died.
Following such notification, the Commissioner must identify whether the organisation remains eligible to hold the contract. Where the organisation is no longer eligible to hold a contract and the issue is not rectified in accordance with any provisions allowing rectification in the contract, the Commissioner must terminate the contract. Please refer to Chapter 11 ‘Contract Terminations and Sanctions’ for more information.
12.6 Practical Issues Arising from Death of a Contractor
12.6.1 Request to form a partnership
Where a GDS contract is held by an individual (whether because of the death of a partner or otherwise), that individual may propose to practice in partnership with one or more persons during the existence of the contract. Please refer to Chapter 4 ‘Contract Variations’ for more information on the relevant process and obligations of the Commissioner.
12.6.2 Procuring a new contract
Prior to the completion of the continuation, the Commissioner will need to decide whether to procure primary care dental services to replace the contract. Any procurement process for a new contract should be completed within the continuation period to allow for continued provision of service.
12.6.3 Considering requests to continue the contract
Where the Commissioner receives a request from the deceased Contractor’s personal representatives to extend the contract, before the end of the initial 28-day period it must:
- seek assurance that the dental staff employed are on the national performers list and have the appropriate qualifications and training to provide all mandatory and additional services under the contract;
- ensure the deceased Contractor’s personal representatives agree that any course of dental treatment started within the agreed continuation period must be completed prior to termination of the contract;
- ensure that the deceased Contractor’s personal representatives agree that:
- where there is an open course of orthodontic treatment, all endeavour is taken to complete the patient’s care during the agreed continuation period; and
- at an agreed date during the agreed continuation period, they will communicate with patients, as appropriate, and as agreed with the Commissioner, that:
- the practice will be under new ownership and a new Contractor will be delivering services; or
- that the practice will be closing/ceasing to offer NHS dental services with patients signposted to local dental practices that are accepting NHS patients and/or referred to NHS 111;
Time frames for communication with patients are largely dependent upon the length of contract/agreement continuation and the circumstances and impact that this would have on service delivery to patients – for example a contract novation or a contract continuing with a partner would not have a financial impact on a patient in terms of additional patient charges but would mean that their dentist may or would change.
Once a contract continuation period has been agreed, the Commissioner will need to amend the existing contract to reflect the continuation period of the contract and work with NHSBSA to make all relevant changes to the payment and contract systems. Changes may vary in individual circumstances to allow the deceased Contractor’s estate to access any NHS Pension rights and for payments to continue to be made under the contract. Advice will need to be taken from both NHS Pensions and NHSBSA and the processes followed as advised by them.
12.6.4 If the practice is to be sold/transferred to a new Contractor
Whilst the deceased Contractor’s personal representatives have the right to sell the practice to any prospective buyer. The Commissioner must make the deceased Contractor’s personal representatives aware that the NHS contract cannot be sold with the practice.
The Commissioner may consider a contract novation to a new provider if all three parties agree. The three parties would be the Commissioner, the deceased Contractor’s personal representatives and the prospective buyer. The Commissioner needs to be aware that novation may lead to challenge. Please refer to Chapter 5 ‘Body Corporates – Variations and Incorporations’ for more information on contract novation.
12.6.5 Non-Continuation or Termination of the Contract
Where the deceased Contractor’s personal representatives do not agree to continue the contract, patients will need to seek another dentist. The Commissioner will need to work with those patients who are currently undergoing a course of treatment to secure alternative provision. There may be a financial impact on patients who may need to pay for the completion of their course of treatment by an alternative Contractor as detailed within section 11.4.1. Commissioners may, with prior agreement of the new contractor, waive any relevant patient charges.
A plan to communicate with patients will need to be discussed and agreed between the Contractor /Contractor’s representatives and the Commissioner.
12.6.6 If the practice is to be closed or the contract is terminated
Under current contractual arrangements practices do not have registered patient lists and are only responsible for patients in an active course of treatment. The processes for the management of these patients are below.
The Commissioner should ensure that it is able to signpost any patients seeking treatment, to other local dentists accepting NHS patients. This may be through making information available at the practice or via the NHS 111 service, whichever is relevant.
12.6.7 For patients who are currently undergoing a banded course of treatment
The deceased Contractor’s family or personal representative(s) must make every effort to complete patients’ treatments within the 28-day period. Where this is not possible for whatever reason, the Commissioner will need to work with other local dental providers to secure completion of the active courses of treatment.
Patients seeking recourse under free repair and replacement provisions need to be made aware that there will be a fee to pay if a repair and/or replacement treatment is performed by an alternative practice; or a continuation of treatment at the same or lower band within two months is needed they will be required to pay the relevant dental charge when this is carried out by another Contractor.
12.6.8 For patients who are part way through an orthodontic course of treatment
Where a patient is undergoing an orthodontic course of treatment, it is unlikely due to the nature of treatment patterns and their longevity, that treatment can be completed within the 28-day period. The Commissioner should work with the Contractor’s representatives to:
- obtain copies of any orthodontic health records for patients currently in treatment that could then be provided to an alternative provider; and
- obtain patients’ details so that they can be contacted regarding continuation of their treatment.
The Commissioner will need to secure alternative provision for those patients undergoing a course of orthodontic treatment. This can be with other local orthodontic providers, or they may need to consider commissioning these services from secondary care providers where alternative primary orthodontic care provision is not available.
Currently the GDS contract or PDS agreement and the relevant Statement of Financial Entitlements state the level of payment for an orthodontic course of treatment. Due to the payment structure and length of an orthodontic course of treatment, the Commissioner may wish to raise the cost pressures of paying for these patient transfers within its risk register. Payments should be made in accordance with Chapter 9 ‘Orthodontic Close Down Arrangements’.
The Commissioner may wish to procure additional activity from orthodontic providers on a non-recurrent basis, on a case-by-case fee structure while they consider whether or not to procure a contract or agreement. If this is the path that is chosen by the Commissioner, it would be advisable to seek independent procurement and legal advice.
Where the contract is not continued, the Commissioner will need to terminate the existing contract and should follow Chapter 11 ‘Contract Terminations and Sanctions’.
13. Managing disputes
13.1 Introduction
This chapter describes the process to determine the action required when a Contractor has requested to follow the NHS dispute resolution process or where the Commissioner elects to follow the NHS dispute resolution procedure.
As decisions made in relation to the contract and its applications can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
This policy focuses on primary dental care contracts in their various forms.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 13.1: Process for managing disputes
- Annex 13.2: Example acknowledgement letter
- Annex 13.3: Example invitation letter
- Annex 13.4: Example Stage 1 Outcome letter (NHS Resolution referral)
- Annex 13.5: Example Stage 1 outcome letter (matter(s) resolved)
13.2 NHS or non-NHS contracts
An NHS contract (as set out in section 9 of the NHS Act) is an arrangement under which one health service body arranges for the provision of goods or services to it by another health service body. It must not be regarded as giving rise to contractual rights or liabilities.
A non-NHS contract is where the contract is legally binding.
In order to appropriately manage disputes the Commissioner must identify whether the contract is an NHS contract or a non-NHS contract. The Commissioner can do this by reviewing clause 14 of the standard GDS contract and PDS agreement. Contractors have the right to be regarded as a health service body under regulation 9 of the GDS Regulations or regulation 9 of the PDS Regulations.
Where a Contractor is regarded as being a health service body, its contract will be an NHS contract. Where a Contractor is not regarded as a health service body, its contract will not be an NHS contract, and therefore is a civil contract. Health service body status affects the eligibility and application process for NHS dispute resolution.
13.2.1 Dispute resolution
There are two different routes that can be taken for resolving contractual disputes, depending on the Contractor’s health service body status:
- Where the Contractor is a health service body, and the contract is an NHS contract the steps laid out in this policy will be used to resolve all matters of dispute. The parties should not make a claim at Court in relation to the contracts.
- Where the Contractor is not a health service body and the contract is a non-NHS contract, the dispute can either be resolved using the process described within this policy or using the Court system.
The use of the Court system can be an expensive and public route. In normal circumstances, non-health service bodies will elect to follow NHS dispute resolution. The Commissioner can request to use the NHS route, but the Contractor does not have to agree, and can choose either route (but that once started down a route it cannot be changed).
Where the parties have followed this policy and NHS dispute resolution to the end determination, the result is binding. A second referral to the Court system for a further ruling on the same issue cannot be made other than to enforce the decision as having the status of a County Court Judgement or to seek Judicial Review of the process.
13.3 Record keeping
It is essential that the Commissioner maintains accurate and complete written records of all discussions, including notes of telephone calls and correspondence on the contract file in relation to the dispute at all levels of dispute resolution. The records should include the dates of communications and who was involved from both parties. The Commissioner should ensure that it responds to Contractor concerns and communications in a timely and reasonable manner.
The table set out in Annex 13.1 provides the steps to be taken in managing disputes.
13.4 Managing disputes – informal process
The GDS and PDS regulations state that the parties must make every reasonable effort to communicate their issues in relation to decision-making and rationale and must co-operate with each other to resolve any disputes that emerge informally before considering referring the matter for determination through formal dispute resolution procedures.
The use of an informal resolution process helps develop and sustain a partnership approach between the Contractor and the Commissioner.
The informal process may include (but is not limited to):
- telephone communications;
- face-to-face meetings at a mutually convenient location;
- virtual meetings; and/or
- written communications.
Most disputes should be able to be resolved at the informal stage, and either party may wish to involve the LDC to help achieve resolution. The formal process should not be initiated until the informal process has been exhausted.
13.5 Managing disputes – Stage 1 (local dispute resolution)
The timescales set out in this stage 1 are indicative only. The Commissioner should ensure any timescales used are appropriate to the circumstances. Regardless of timescales, the parties must ensure that every reasonable effort to communicate and co-operate with each other is made prior to invoking stage 2 of the NHS dispute resolution procedure.
Where a dispute arises, the Commissioner should refer to the relevant policy that covers the issue that caused the dispute to determine whether due process has been followed.
The Contractor should notify the Commissioner of its intention to dispute one or more decisions made in relation to its contract. This notification should be received no later than 28 days after the Commissioner advises the Contractor of its decision except in exceptional circumstances.
The Commissioner will immediately cease all action in relation to the disputed notice or decision, until:
- there has been a determination of the dispute and that determination permits the Commissioner to impose the planned action; or
- the Contractor ceases to pursue the NHS dispute resolution procedure or Court proceedings, whichever is the sooner.
However, where the Commissioner is satisfied that it is necessary to terminate the contract or impose a contract sanction before the NHS dispute resolution procedure is concluded to:
- protect the safety of the Contractor’s patients; or
- protect the Commissioner from material financial loss,
then the Commissioner shall be entitled to terminate the contract or impose the contract sanction at the end of the period of notice it served. This should only be followed with close reference to the GDS Regulations and PDS Regulations, pending the outcome of that procedure.
13.5.1 Process for stage 1 (local dispute resolution)
The paragraphs below set out a process that may be adopted for stage 1 (Local Dispute Resolution). Within the commissioning team the person(s) undertaking the local dispute resolution process must not be the same person(s) who were involved in the decision-making process on the issue that is being disputed.
The Commissioner must acknowledge, in writing, the notification of dispute within seven days of receipt. This acknowledgement letter will include a request for the submission of supporting evidence from the Contractor within a further 28 days from the date of the acknowledgement letter. An example acknowledgement letter is provided in Annex 13.2.
Upon receipt of the evidence the Commissioner should review the evidence within 28 days and invite the Contractor to attend a meeting, which should be as soon as possible, but at the very latest within a further 28 days. This meeting can be held virtually or on a face-to-face basis. The Contractor(s) can invite representative bodies to support it at the meeting, for example, the LDC. An example invite letter is provided in Annex 13.3.
Once the meeting has been held, the Commissioner should notify the Contractor in writing of the outcome of the meeting, whether this is that the dispute will now need to be moved to stage 2 of the NHS dispute resolution procedure. An example stage 1 outcome letter is provided in Annex 13.4, or alternatively that the dispute has been successfully resolved. Please refer to the example stage 1 outcome letter in Annex 13.5.
Where the matter is resolved the issue can now be deemed as closed and the Commissioner should document the outcome accordingly on the contract file. All records of the dispute should be retained on the contract file.
Where the matter remains unresolved, the process may be escalated to the next stage of the dispute resolution procedure. At this point the Commissioner should commence preparation of the contract file to ensure that when NHS Resolution or court requests submission of evidence in respect of the dispute the documentation is in order.
13.6 Managing Disputes – Stage 2 (NHS Dispute Resolution Procedure)
The informal process and stage 1 (Local Dispute Resolution) must be exhausted before proceeding to this stage of the process. The Commissioner or a Contractor wishing to follow this route must submit a written request for dispute resolution to NHS Resolution, which carries out the NHS dispute resolution functions of the Secretary of State in the GDS Regulations and the PDS Regulations. The written request must include:
- the names and addresses of the parties to the dispute;
- a copy of the contract; and
- a brief statement describing the nature and circumstances of the dispute.
The request should also include:
- what the applicant sees as the appropriate outcome of the dispute; and
- confirmation that all local dispute resolution options have been exhausted.
Further information on the details that should be provided within an application for dispute can be found in NHS Resolution’s guidance note that was issued in March 2021.
The written request for dispute resolution must be sent within a period of three years from the date on which the matter gives rise to the dispute occurred or should have reasonably come to the attention of the party wishing to refer the dispute.
The Commissioner will be required to prepare documentation, evidence and potentially an oral presentation in response to evidence presented in support of the dispute.
When providing the evidence for NHS Resolution the Commissioner should:
- meet all deadlines set out by NHS Resolution
- clearly set out the viewpoint of the Commissioner
- provide a chronology of events including
- the Commissioner’s decision
- the point at which the decision was made
- the rationale for the decision
- the consideration of alternative approaches
- always provide documentation which supports the approach taken by the Commissioner and reference this.
The parties should not underestimate the preparation that may be necessary in the event that evidence is required by NHS Resolution, as all records pertaining to the Contractor may be required by NHS Resolution, including (but not limited to) all contract documentation and contract variations, all written correspondence (both to and from the Commissioner and the Contractor) and any electronic correspondence that may have passed between the parties, in relation to the dispute. This process will benefit from a clearly recorded contract file.
Each party will be asked to prepare representations on the dispute, which will be circulated to the other party and an opportunity to provide observations on the other party’s representations will be given. Again, the observations of each party will be circulated to the other party.
The Commissioner must ensure that records of communications and contract files are maintained to a high standard and all documentary evidence is collated correctly prior to submission to NHS Resolution.
Once NHS Resolution has reached a conclusion (the determination) the parties will receive a copy and will be required to act upon it. Following a determination in late 2020 by the Court of Appeal, NHS Resolution will consider awarding interest in relation to costs associated with the appeal. However, NHS Resolution will only consider awarding interest if claimed by a party when the application for dispute resolution is lodged or raised by the other party. Further guidance can be found on this on NHS Resolution’s website.
Please refer to the NHS Resolution guidance for further information on the process. The link to this document is given in paragraph two of this section.
NHS Resolution publishes up to three years’ worth of past decisions on its website, which includes the considerations and determinations of each case. These can be found on the NHS Resolution’s website.
13.7 Other Dispute Resolution Procedures
Where the Contractor is not a health service body and raises a dispute via the court system, the Commissioner will need to respond to communications via the Contractor’s solicitors.
The Commissioner may also raise a dispute with the Contractor and will need to follow the processes outlined above.
Disputes may also arise prior to a contract being entered into. Such disputes may relate to the eligibility of the person seeking to enter into the contract or contract terms.
Where the Commissioner is of the view that a person seeking to enter into a contract does not meet the eligibility conditions of Regulations 4 or 5 of the GDS Regulations or the PDS Regulations, the Commissioner must notify the person in writing.
This notice must state the Commissioner view of the person’s eligibility, the reasons for that view and guidance on the person’s right of appeal.
Where the Commissioner has issued such a notice, the recipient of the notice has a right of appeal to the First-Tier Tribunal (Care Standards) Further information can be found on the GOV.uk website.
Where the dispute relates to the parties being unable to agree on a particular proposed term of a GDS contract or PDS agreement, either party may refer the dispute to the Secretary of State to consider and determine the matter in accordance with:
- For GDS contracts, paragraphs 55(4) to 55(13) and 56(1) of
Schedule 3 and paragraph 8(5) of the GDS Regulations; or
- For PDS agreements, 55(4) to 55(13) and 56(1) of Schedule 3 and paragraph 8(4) of the PDS Regulations, except where both parties to the prospective agreement are health service bodies (in which case section 9 of the NHS Act applies).
14. Adverse events
14.1 Introduction
Adverse incidents are dealt with in the force majeure provisions of the standard GDS contract and PDS agreement. Although these provisions are not required by the GDS Regulations or the PDS Regulations, the majority of GDS contracts and PDS agreements will include them.
The Commissioner is advised to check that the force majeure provisions are included in each contract and if they are to follow the guidance in this policy. This policy is only applicable where the contract in question has retained the recommended force majeure provisions.
The Contractor is responsible for informing the Commissioner of any force majeure event promptly and no later than five working days of the occurrence of such circumstances or events and for lodging a claim for relief within the timescales specified within this document.
The Commissioner is responsible for advising Contractors of the outcome of any claim once processed and applying that relief to the Contractor’s contract by way of carry forward activity on the payment and contract systems.
As decisions made in relation to the contract and its applications can be disputed, it is essential that the Commissioner has robust processes in place for decision making. This includes maintaining thorough and accurate records of all communications, discussions, and actions. The decision-making process should be clear, and any decision or contractual notice should be taken and communicated at an appropriate level as per organisational processes or local scheme of delegation.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 14.1: Contractor’s preliminary notice of force majeure event
- Annex 14.2: Acknowledgement of receipt of preliminary notice of force majeure event form
- Annex 14.3: Claim form for dental relief
- Annex 14.4: Template for calculating lost activity (dental relief)
- Annex 14.5: Notification to Contractor on outcome of claim for dental relief – approved
- Annex 14.6: Notification to Contractor on outcome of claim for dental relief – declined
14.2 Contract wording
Clause 372 to 375 of the GDS contract and clauses 350 to 353 of the PDS agreement provide that:
‘Neither party shall be responsible to the other for any failure or delay in performance of its obligations and duties under this Contract which is caused by circumstances or events beyond the reasonable control of a party. However, the affected party must in the occurrence of such circumstances or events:
- inform the other party in writing of such circumstances or events and of what obligation or duty they have delayed or prevented being performed; and
- take all action within its power to comply with the terms of this Contract as fully and promptly as possible.”
Unless the affected party takes such steps, [the clause above] shall not have the effect of absolving it from its obligations under this Contract. For the avoidance of doubt, any actions, or omissions of either party’s personnel or any failures of either party’s systems, procedures, premises, or equipment shall not be deemed to be circumstances or events beyond the reasonable control of the relevant party for the purposes of this clause, unless the cause of failure was beyond reasonable control.’
14.3 Force Majeure Event
A force majeure event is one which is caused by circumstances beyond the reasonable control of either the Commissioner or the Contractor that could not have been avoided or mitigated with reasonable care and where the event has had a material effect on the fulfilment of the contract.
Examples of events that may invoke the force majeure provisions are as follows:
- fire;
- flood;
- severe weather conditions and for which precautions are not ordinarily taken to avoid or mitigate the impact (for example a severe hurricane);
- industrial action which significantly affects the provision of public services or services upon which the party is reliant;
- death of a significant performer or close relative (for the purposes of this policy. a close relative is defined as, mother, father, sister, brother, wife, husband, civil partner, daughter, son, grandparent, grandchild, parent-in-law, son-in-law, daughter-in-law, sister-in- law, brother-in-law, step-parent, step-child, step-sister, step-brother, foster child, legal guardian, domestic partner or fiancé/fiancée);
- pandemic disease or circumstances that might otherwise be considered “an act of God”;
- war;
- civil war (whether declared or undeclared);
- riot or armed conflict;
- radioactive, chemical, or biological contamination;
- pressure waves caused by aircraft or other aerial devices travelling at sonic or supersonic speed;
- acts of terrorism; and/or
- explosion.
14.4 Dental relief
Throughout this policy the term dental relief is used. This is used as an outcome measure that will effectively determine the total units of activity that the Contractor was delayed or prevented from providing during the force majeure period and which may be ‘carried forward’ to the following financial year, instead of the Commissioner recovering the overpayment in respect of the UDAs/UOAs not provided.
The Commissioner’s decision whether to grant dental relief will be based on the assessment of a Contractor’s claim for relief, where there has been an inability to deliver the contractual activity required. This policy provides the template documents that are relevant to the process of assessing eligibility for and granting dental relief, and also sets out the criteria, processes, and examples of what would constitute a force majeure event. There is also a calculator and methodology provided for calculating the amount of dental activity that can be carried forward.
If the Commissioner is satisfied that a force majeure event occurred and all reasonable efforts have been made to mitigate the consequences of the force majeure event, it may allow the Contractor to carry forward to the following financial year a number of unfulfilled UDAs or UOAs which, it is estimated, were not delivered as a direct result of the force majeure event. It is expected that any activity carried forward will be delivered within the next financial year.
Neither the standard GDS contract or PDS agreement make provision for financial compensation or dispensation to be awarded to the Contractor, so ‘carry forward’ activity will be permitted where it is felt that the force majeure event impacted on the Contractor’s ability to deliver their contractual obligations.
In order to be considered for dental relief a Contractor must have followed the correct procedure of notifying the Commissioner, which is detailed below, promptly, and no later than five working days of the occurrence of the force majeure event and must have submitted the claim form that is provided in Annex 14.3.
If a Contractor is claiming for dental relief, the Commissioner should postpone consideration of the issue of a Remedial or Breach Notice for under-delivery until the outcome of the claim is known. Where the claim is successful, it is inappropriate for the Commissioner to issue a Breach or Remedial Notice for under-delivery. For audit purposes the Commissioner will need to ensure local governance processes are followed.
14.5 Circumstances of Force Majeure Event
In considering claims for dental relief, it is important to consider the event and the point in the financial year when it took place.
Claims for relief in respect of planned or anticipated events should not be considered because whilst they may affect service delivery in the short term, the Contractor is required to deliver the activity during the relevant financial year. The Contractor is expected to plan its own delivery (within the requirements of the contract) and should plan for anticipated events that might affect the day-to-day delivery of units of activity (i.e. additional bank holidays).
It is entirely reasonable to expect a Contractor to make arrangements to ensure that activity lost through an unplanned event occurring at the beginning or middle of the financial year is recovered and the contracted activity is delivered in full by 31 March, and in all circumstances can be accommodated within the 4% tolerance of delivery of activity.
14.6 Possible Events or Circumstances for Dental Relief Claims
The following is a list of examples of events or circumstances where the claim for relief may be considered, but it is not exhaustive.
14.6.1 Death of a performer or individual provider
In these circumstances it is understood that there may be a temporary interruption of services while arrangements are put in place to secure the successor to the business and/or engage the services of a clinician to resume service provision. Please refer to Chapter 12 ‘Death of a Contractor’ as this provides clarity around contract continuations, even when held by a single-handed Contractor.
14.6.2 Death or sudden serious illness of a close relative or a significant performer
Death or sudden illness of a close relative or a significant performer which could result in an inability to:
- fill the post; or
- make up shortfall in activity by year end.
For the purposes of this policy, sudden serious illness or ill health means an illness or accident causing significant disability. Examples of such illnesses include (but are not limited to) myocardial infarction, CVA or cancer. In the case of a significant performer, sudden serious illness or ill health means illness that is such that the performer is unable to work for a period which is likely to substantially impact on productivity
14.6.3 Significant period of absence due to accident or sudden serious ill health of a significant performer
If a performer responsible for a significant proportion of the contracted activity is suddenly taken ill and is unable to deliver the services for a significant period of time, the Commissioner may consider that this is a circumstance for which relief may be considered.
14.6.4 Physical damage to premises
Physical damage to premises from which the dental service is delivered rendering it impossible and/or an unsafe environment from which to deliver care over a period, such as the following:
- fire causing significant damage which prevents the premises from being used over a prolonged period; or
- flood causing significant damage which prevents the premises from being used over a prolonged period.
14.6.5 Essential services failure
For example, in the event of a power failure or the water supply being turned off rendering it impossible for the dental services to be provided.
14.6.6 Pest infestation
Where the infestation would render the delivery of the service impossible from the premises, where the premises must be closed for a period to treat the infestation and/or repair damage that has been incurred.
14.6.7 Significant adverse weather
Significant adverse weather for which precautions are not ordinarily taken to avoid or mitigate the impact and which result in damage to the premises which prevent their use over a period of time (minimum three-week period), such as following a hurricane.
14.6.8 Prolonged industrial action
Industrial action over a prolonged period of time which significantly affects the provision of public services or services upon which the Contractor is reliant.
14.7 Unacceptable events or circumstances for dental relief claims:
The following is a list of examples of events or circumstances where the claim for relief should not be considered. It is not exhaustive.
14.7.1 Refurbishment of premises
It is expected that Contractors are able to deliver a high standard of quality care from premises which meet the requirements of the CQC and all relevant legislation. Premises should also meet the requirements of infection control and decontamination as detailed in the Health Technical Memorandum 01-05(Decontamination in primary care dental practices) produced by the Department of Health. Claims in respect of interruption to service as a result of refurbishment or renovation will not be considered as relevant circumstances in which relief should be given for failure of contractual obligations.
14.7.2 Adverse weather
Severe weather in the UK, particularly during the winter months when snow and ice may be prevalent for varying periods of time, is considered normal and therefore does not constitute exceptional circumstances for which Contractors may be given relief, regardless of any inconvenience it may cause.
14.7.3 Planned events
A performer’s elective surgery, annual leave, weddings, and similar events are occurrences for which prior notification is always required. They are by their nature planned events and it is expected that the Contractor will make the necessary provision to ensure the service continues to be delivered in the absence of the relevant performer.
14.7.4 Long term sickness causing some incapacity disability, maternity, paternity, or adoption leave of a performer
Long term sickness causing some incapacity disability, maternity, paternity, or adoption leave of a performer.
The term long term “sickness is often applied when the course of the disease lasts for more than four weeks. An example of long-term sickness includes but is not limited to, cancer, inflammatory arthritis, and severe and enduring mental illness.
It is expected that the Contractor will make necessary provision for the continuation of the service in the performer’s absence. Contractors are advised to refer to the relevant SFE for information about payments in respect of long-term sickness, maternity, paternity, and adoption leave.
14.8 Process for claiming dental relief
On receipt of a notification from a Contractor that a force majeure incident has occurred, the Commissioner will send the Contractor an electronic copy of the formal preliminary notice of force majeure that is contained within Annex 14.1.
The Commissioner will also explain the process for making a claim for dental relief at year end.
On receipt of the completed preliminary notice form from the Contractor, the Commissioner will review the preliminary notice against the force majeure criteria, and will send the Contractor the acknowledgement of Contractor notification letter based on the template contained at Annex 14.2, and the template claim form at Annex 14.3 advising the Contractor that it must submit its claim for relief using the template claim form by the date specified in the letter. It is the responsibility of the Contractor to submit a claim and not for the Commissioner to request or chase a claim.
If on receipt of the completed preliminary notice from the Contractor, the Commissioner determines that it does not meet the criteria, the Commissioner will advise the Contractor at that point (rather than wait until year end). Annex 14.6 can be adapted and used for this purpose.
Any claims must be submitted using the template provided at Annex 14.3.
The template must be completed in full providing details of the force majeure event, the impact on service delivery, the period over which service was interrupted and the action taken to mitigate the impact of the event. The claim template must be accompanied with supporting evidence for the Commissioner to assess and award any relief. See Section 14.9 below for further information on the evidence to be provided.
On receipt of each claim the Commissioner will check for completeness and allow five working days for the Contractor to clarify or provide additional information or supporting evidence as requested. The Contractor should be advised that if the requested information is not forthcoming by the due date the claim may not be considered.
The Commissioner will record the status of the claim and acknowledge receipt of the claim. It will also notify the Contractor of the date by which they may expect to be advised of the decision.
The Commissioner will assess the evidence provided in the claim and make a decision on whether or not to award relief on the basis of this. If a decision is made to award a claim for dental relief, the level of relief to be provided should be determined using the template calculator provided in Annex 14.4. Any discussions and decisions taken must be formally recorded and signed off by the relevant person within the Commissioning team. The decision should be communicated to the Contractor using the template letters provided in Annex 14.5 and Annex 14.6 by the date specified by the Commissioner when it acknowledged receipt of the claim.
If the Contractor’s claim for dental relief is successful, then the issue of Remedial Notice or Breach Notice is to be waived by the Commissioner. For audit purposes Commissioners will need to ensure local governance processes are followed.
14.9 Evidence
Contractors must provide evidence of the force majeure event and the impact that it has had on service provision when they submit their claim at year end.
Examples are as follows:
- copy of a death certificate;
- letter from the treating medical professional, hospital, or treatment centre, confirming the diagnosis or condition of the performer in question and the period for which it considers the individual should be absent from work;
- photographs of damage to premises, dated invoices or estimates for repair, photocopy of daybook evidencing the premises closure; and/or
- written confirmation from a utilities company regarding service being cut off due to the force majeure circumstances.
Following the review of any claim for dental relief, the Commissioner should return any supporting personal information to the Contractor or agree to dispose of it appropriately.
14.10 Contract compliance
Contractors are required under the terms of their contracts to promptly notify the Commissioner (which for the purposes of this policy is within five working days) of a force majeure event, detailing the cause or event, what service provision is being delayed or prevented and what action(s) within their power they are taking in order to comply with the terms of the contract as fully and promptly as possible. Submitting at year end claim form.
Failure to notify the Commissioner will mean that the Contractor is not absolved from its obligations under the contract and will render any claim for dental relief invalid. This may mean that the Contractor is in breach of its contract because of under delivery of its contracted activity which will not be mitigated against as a result of the force majeure event occurring.
Neither party will be responsible to the other for any failure to delay in performing its obligations and duties under the contract which is caused by an event of force majeure.
14.11 Clinical governance and risk management/termination
If the consequence of the Contractor’s failure to deliver services is significant and poses a risk to patient safety or the efficiency of wider primary care services, the Commissioner may wish to consider recording the incident on the risk register or invoking its termination rights.
If the service provision is delayed or prevented for a continuous period of three months, then either party may terminate the agreement by notice in writing within a period which is reasonable (and no less than 28 days) This termination will not take effect where the service is resumed within the period of notice or if the Contractor consents to this.
14.12 Claims for relief
Claims for relief cannot be considered until the year end data (produced by the NHSBSA) has been released to both the Contractor and the Commissioner. It is the responsibility of the Contractor to submit a claim for relief and not for the Commissioner to pursue this with the Contractor.
On receipt of claims for relief the Commissioner should consider the following:
- Was the Commissioner advised promptly of the event using the template provided?
- Were there satisfactory business continuity plans in place to help mitigate the consequences of the force majeure event?
- Was it demonstrated that all steps that were reasonably practicable were taken to ensure continuity of patient care during the period in relation to which relief is being claimed?
14.13 Calculating dental relief
Calculation of the appropriate level of relief that a Contractor is awarded should be based on the activity that the relevant performer(s) would normally deliver in a day. This should be evidenced based and recorded on the claim form by the Contractor.
Reference should therefore be made to the report produced by NHSBSA at year end entitled ‘Year-end Statement of Activity’ which identifies activity (including amendments) collected from FP17s in any of the fifteen schedule months from 1 April to 30 June, where the date of completion of a course of treatment is between 1 April and 31 March (inclusive). This report identifies the activity delivered by every performer listed under the contract in the full financial period.
Calculation of dental relief should take account of the number of working days the performer(s) has been engaged in delivering NHS dental care under the contract during the financial period, which will exclude the days that the performer could not work due to the force majeure event. If employed for a full financial year this equates to 240 days. So, for example, in the case of a performer who has worked full time from 1 April to 31 March and delivered 3000 UDAs/UOAs, the estimated daily average will be 12.5. (3,000 / 240 =12.5).
If they did not work for a period of five days because of the force majeure event, the lost activity is calculated to be 62.5 UDAs/UOAs. (5 *12.5 = 62.5). This would be calculated pro rata for a part time performer. There is a template for calculating lost activity provided in Annex 14.4.
Where the Contractor’s whole practice is closed then the total UDAs/UOAs delivered divided by the number of days the practice was open would provide the daily amount. The Commissioner should remember that some dental practices are only open or provide NHS care for part of the week.
14.14 Appeals
If on consideration of the information and evidence provided, the Commissioner does not approve the claim for dental relief, the Contractor has the right to appeal, firstly through the local dispute resolution process.
The parties should refer to Chapter 13 ‘Managing Disputes’ for the process in relation to disputes.
14.15 Payment and contract system
The Commissioner will need to record any carry forward activity that was granted on the payment system and contract file.
Where dental relief is not granted, a repayment plan needs to be agreed, in writing, between the Commissioner and the Contractor and detailed on the payment system and contracts file.
The parties should discuss the effect of force majeure on payments by the Commissioner to the Contractor. The Commissioner should use its reasonable discretion in determining payments regarding the need for the Contractor to continue to provide services once it is no longer affected by the force majeure event provided the contract has not been terminated.
15. Practice closedown
15.1 Introduction
There are several reasons why a practice may close down and cease to provide NHS primary dental services. These can broadly be summarised into two main categories: planned and unplanned.
The reasons that a practice may close include:
- the time-limited contract coming to an end;
- being terminated by either the Commissioner or the Contractor. Further information on this can be found in Chapter 11 ‘Contract Terminations and Sanctions’;
- an adverse event. Further information this can be found in Chapter 14 ‘Adverse Events’;
- the death of the Contractor. Further information on this can be found in Chapter 12 ‘Death of a Contractor’;
- retirement of the Contractor. Further information on this may be found in Chapter 4 ‘Contract Variations’.
This policy outlines the approach when dealing with both planned and unplanned closures.
Several supporting documents and templates are provided in the accompanying appendices document for this chapter:
- Annex 15.1: Guide to communication with Contractors
- Annex 15.2: Checklist for documentation recording when contract ends
- Annex 15.3: Template detailed report structure
- Annex 15.4: Template exit plan
- Annex 15.5: Template operational management plan
- Annex 15.6: Template letter for patients’ records management for closing practice – UDA practices
- Annex 15.7: Template letter for patients’ records management for closing practices – UOAs
- Annex 15.8: Template letter further to Contractor’s letter of termination
- Annex 15.9Contract hand back template letter for patients with frequently asked questions
- Annex 15.10: Contract hand back communications and engagement plan
15.2 Planned closures
15.2.1 Time limited contracts coming to an end
Time-limited contracts can be in place for GDS contracts and PDS agreement types. GDS contracts, however, do not usually have an end date but it is possible for an urgent temporary GDS contract to be put in place for a period not exceeding 12 months, for the provision of services to the former patients of a Contractor following the termination of that Contractor’s contract. Further information on urgent contracts can be found in Chapter 3 ‘Which Dental Contract When?’
PDS agreements may be in perpetuity or for a time limited period. Commissioners should review the relevant PDS agreement to establish if there is a defined end-date.
In each of the cases above there are generic principles that will apply and individual circumstances that will need to be considered. This policy covers the steps to be taken in advance of the end of any contract and will support the Commissioner in planning procurement cycles and future service provision.
The Commissioner must consider whether the expiring contract contains provisions relating to the end of the contract that impact on any practice closedown actions. The standard GDS Contract contains provisions relating to the consequences of termination including a requirement that the Contractor co-operates with the Commissioner and arrangements for a financial reconciliation exercise.
15.3 Timetable for managing contracts coming to an end
The Commissioner needs to be aware of the end dates of all contracts held so that advance planning can be undertaken to ensure both capacity and timescales can be aligned with the key stages outlined below.
It is essential that the Commissioner ensures continued communication with Contractors throughout the stages to enable them to have a clear understanding of the processes, expectations, and obligations. Annex 15.1 provides a guide to communications with Contractors and Annex 15.2 sets out a proposed checklist for documentation recording.
In each of the stages below there are a range of activities that may need to be undertaken, depending on the Commissioner’s preferred route, and the Commissioner may wish to consult with the appropriate LDC throughout.
15.4 Summary of key stages
There are three key stages:
15.4.1 Stage 1: minimum 9 to 15 months before contract end (all essential):
- needs assessment;
- value for money;
- impact assessment; and
- engagement proposal.
15.4.2 Stage 2: 12 months before contract end:
- notice period – exit plan;
- wind-down of services;
- commence procurement and either:
- begin negotiations for continuation with Contractor; or
- begin exit arrangements of incumbent provider and mobilisation of any new provider.
15.4.3 Stage 3: at contract end:
- arrangements for ongoing treatment of patients under existing course of treatment;
- variation to contract/extension: and
- commencement of new provider.
15.5 Stage 1 – 9 – 15 months before contract end
The considerations that should be given when completing each action are provided below. This list is not exhaustive but does provide a platform for Commissioners to fully assess the existing and future service needs of its population. Commissioners should ensure that all appropriate stakeholders are given the opportunity to input into the needs assessment for their population, including but not limited to public health.
15.5.1 Needs assessment
Is there still a demand for this service in this locality and a requirement for it to continue? For example, to reduce inequalities in access or health outcomes
- Does the contract specification still address current local priorities?
- Has the contract delivered on the expected outcomes?
- Has the service provided added value to the local population and service provision?
- Have you assessed the potential service needs for a forthcoming new development?
- What is the capacity of other local providers and the market for other providers to deliver services?
- Have you given consideration to any specialist services needs in the locality?
- Are there any needs which are not met by the contract which could be delivered?
15.5.2 Value for money
Have you considered all available outcome and delivery data held nationally and locally, regarding the current service and impact on other providers?
Have you compared the cost of the current service against other providers i.e. cost per head of population whilst taking into account any differences in the scope of the services provided?
- is the current service still affordable within projected future budgets?
- has the contract delivered on the expected financial outcomes?
- what other objectives might be set within the existing budget?
15.5.3 Impact assessment
- Have you considered the potential impact on service users/patients?
- Have you considered the potential impact on other service providers, e.g. GPs, pharmacy, local trust, out of hours, community services?
- Have you considered the potential impact on the current provider, i.e. continued viability within the locality?
- Have you considered patient choice and equality?
- Have you considered the potential risks i.e. reputational (adverse publicity, Commissioner/provider relationship), market testing, timescales and financial?
- Have you considered how the expiry of the contract affects compliance with the general duties of NHS England? For further information on these duties, please refer to Chapter 2- ‘General Duties of NHS England’.
15.5.4 Engagement proposal
Each situation will need to be managed regarding each individual circumstance and the nature of the procurement process to be followed, if at all. However, where it has been deemed appropriate to complete a form of consultation before taking action, the Commissioner should consider whether:
- service users/patients have been involved? Refer to Chapter 2 ‘General Duties of NHS England for more information on this requirement;
- other local providers and other interested parties have been involved i.e. LDC;
- local members of parliament, review, and scrutiny committee, etc. have been consulted?
- the local ICS partners have been consulted?
If the answer is ‘no’ regarding any of the above, the Commissioner should be able to identify the grounds they felt consultation was unnecessary and these should be included in the report defined below.
15.5.5 Completion of Stage 1
Completion of stage 1 will provide all the information required to enable the Commissioner to make an informed commissioning decision on whether to re-commission, procure or allow the service to end. At this stage, the Commissioner should develop a detailed report about the investigations undertaken, consultation and outcomes. A template report structure is available for this purpose in Annex 15.3. This report shall demonstrate that the Commissioner has considered all possible options and the rationale behind the decision taken.
15.6 Stage 2 – 12 Months before contract end
Below are the potential next stages following stage1 based upon the Commissioner’s decision regarding the proposed way forward. It is important to note that where a contract has a duration, or an end date specified, and the intention is to allow the contract to naturally expire, there is no requirement to issue a formal Termination Notice. It would be best practice to issue a formal letter of notice detailing the Commissioner’s intentions and the obligations on the Contractor throughout the remainder of the contract period.
15.6.1 Notice period – exit plan
The Commissioner may wish to issue a letter of notice of intentions.
The Commissioner may wish to develop an exit plan with the Contractor and have clearly defined Commissioner / Contractor responsibilities. A template to support this process is provided in Annex 15.4. This plan should be developed whether the contract is to cease or transfer to a new provider. Commissioner should review the contract and ensure any exit arrangements detailed in the contract are followed.
15.6.2 Wind-down of services
The Contractor should use best endeavours to complete patients’ treatments prior to close-down because, where a continuation of treatment at the same or lower band within two months is needed, patients will be required to pay the relevant dental charge when this is carried out by another provider.
The Commissioner should discuss with the Contractor on a case-by-case basis how the Commissioner will support the transition to a new provider (if applicable).
15.6.3 Procurement
The Commissioner should ensure any new contract is procured in accordance with procurement law. Commissioners must also act in accordance with any procurement protocol issued by NHS England.
Once a preferred provider is established, the Commissioner should agree an operational management plan. A template is provided in Annex 15.5. This template should only be used where the contract does not contain exit arrangements as any such arrangements take precedence over the template.
15.6.4 Begin negotiations for continuation of the contract with the existing Contractor, if appropriate
Extending any contract beyond a previously agreed end date could be considered a material change to the terms of that contract which could lead to a procurement challenge.
If there is no extension period already included in the contract, the Commissioner will need to consider carefully whether such an extension should instead be subject to a full procurement process to ensure best value and mitigate the risk of challenge from previous and/or potential alternative service providers. If the Commissioner’s decision is that no procurement process is necessary, then it must ensure it is aware of the necessary steps which must be taken to satisfy procurement law.
Once the decision to extend has been reached and all correct processes have been followed the Commissioner will need to consider:
- the length of extension;
- any alterations to the existing contract (including the financial arrangements); and
- any agreement of new key performance indicators (KPIs)
15.6.5 Completion of stage 2
Completion of stage 2 will provide the Commissioner with the firm foundations and detailed preparations ready to manage the end of the contract.
15.7 Stage 3 – At contract end
Below are the possible outcomes culminating from stages 1 and 2.
15.7.1 Arrangements for ongoing treatment of patients under existing course of treatment
Where courses of treatment have not been completed, the Commissioner should ensure that patients are aware that where a continuation of treatment at the same or lower band within two months is needed, patients will be required to pay the relevant dental charge when this is carried out by another provider. Similarly, patients seeking recourse under free repair and replacement provisions need to be made aware that there will be a fee to pay if a repair and/or replacement treatment is performed by an alternative practice.
Where a patient is undergoing an orthodontic course of treatment, it may not be possible, due to the nature of treatment patterns and their longevity, that treatment can be completed prior to close-down. The Commissioner should work with the Contractor’s representatives to:
- obtain copies of any orthodontic health records for patients currently in treatment that could then be provided to an alternative provider; and
- obtain patients’ details so that they can be contacted regarding continuation of their treatment.
The Commissioner will need to secure alternative provision for those patients undergoing a course of orthodontic treatment. This can be with other local orthodontic providers, or they may need to consider commissioning these services from secondary care providers where alternative primary orthodontic care provision is not available.
Currently the GDS contract or PDS agreement and the relevant SFE state the level of payment for an orthodontic course of treatment. Due to the payment structure and length of an orthodontic course of treatment, the Commissioner may wish to raise the cost pressures of paying for these patient transfers within its risk register. Payments should be made in accordance with the section on orthodontic close down arrangements in Chapter 9 – ‘Orthodontics’
The Commissioner may wish to procure additional activity from orthodontic providers on a non-recurrent basis, on a case-by-case fee structure while they consider whether to procure a contract or agreement. If this is the path that is chosen by the Commissioner, it would be advisable to seek independent procurement and legal advice.
15.7.2 Contract end
This is the point when the service ceases to be delivered.
Communication to be sent out to all those parties involved e.g. management of patient communication working with provider, management of the press, notification of contract end to relevant stakeholders.
15.7.3 Variation to contract – extension
Contract variation is issued and signed off by both parties.
15.7.4 Commencement of new provider
Issue of new contract.
A operational management plan implemented by the Commissioner.
Relevant communications is undertaken, internally and externally.
On completion of stage 3, the Commissioner will have reached an agreed, structured outcome about the management of contract end.
15.8 Unplanned/unscheduled and unavoidable practice close-down
When a dental practice closes at short notice, it is important that Commissioners respond and act in a timely way. Such closures may be as result of actions by the CQC, for example voluntary closure in response to an adverse inspection or cancellation of the practice’s registration, or due to the sudden inability of a provider to continue providing a service for some other reason such as bankruptcy.
Furthermore, it is critical that the management and transfer of patient records (both paper and digital) are undertaken in a secure and robust manner. It is important that adherence to all applicable information governance, records management and both EU General Data Protection Regulations (GDPR) and data protection principals are maintained throughout this process. Dental practices/contract owners are obliged to ensure the security of all personal data stored, owned, and processed by them. It is the responsibility of the Contractor to ensure that they are always compliant with the requirements of GDPR. This includes when contracts are voluntarily or involuntarily terminated.
15.9 Scope
This policy clarifies the role of the Commissioner and the engagement required with patients and any partner organisations (e.g. NHS England or CQC). This section is intended as guidance for Commissioners, with four fundamental principles at the core:
- The needs of the patients must be at the heart of all decisions and actions
- In many cases taking preventive action in conjunction with support could be a preferable option to closing a practice
- In the circumstances where this section applies (e.g. a closure is unavoidable or in the best interests of patients), all partners and stakeholders should know what to do, when and how, and to work effectively together to minimise any disruption to patients and services
- Communication must be maintained throughout with patients and their families and carers and with other partners (e.g. LDCs / Healthwatch)
15.10 Roles and responsibilities
15.10.1 Commissioners
The Commissioner will take the lead in the following actions:
- ensure appropriate interim measures are put in place to keep patients safe after the identification of concerns or issues or at the very latest, the point it is informed of the closure
- establish a team with specialist skills to oversee the closure, including contracting and communications staff, and lead on arranging meetings/consultations with any partners
- establish a task and finish group to oversee the process
- communicate to patients the details of alternative dental practices which could provide mandatory services
- maintain ongoing consultative relations with patients, their families, other local dental practices, and any other system partners to ensure they are kept informed at each step of the process
- commission new services and arrange people to move and resettle, including a review of the placement after a reasonable timeframe subject to local commissioning intentions
- identify a lead to coordinate communications
- engage with Local Dental Committee (LDC)
If the practice physically closes, the Commissioner will:
- put in place arrangements for practice post to be redirected to the Commissioner and where appropriate make a personal visit to the premises
- ensure call forwarding arrangements are in place or appropriate answerphone message are established for the closing practice to alert patients and inform NHS 111, OOH services
Dental Practice (during any period where the practice is still open):
- The Commissioner will ask the dental practice to:
- assist with ensuring appropriate interim measures are put in place to keep people safe after the identification of concerns
- assist the Commissioner with the assessment of, and communication, with residents and their families to ascertain their needs and preferences
- assist the Commissioner in any patient engagement, in particular those with people accessing services provided at or by the dental practice and their families
- review and act on any guidance provided by the Commissioner in relation to the closure
- Record, collate and remove prescription pads. This includes both handwritten and computer scripts
- ensure all drugs/medicines in the practice are noted and handed into the local pharmacy and signed for
- ensure that they are always compliant with the requirements of General Data Protection Regulations (GDPR) in relation to patients’ records. A template letter for Commissioners to send to providers can be found in Annex 15.6 for UDA practice and Annex 15.7 for UOA practices
15.10.2 Care Quality Commission (CQC)
CQC will lead in the following actions:
- Share with the Commissioner any information held about the quality of the current service.
- Share with the Commissioner any information held about the quality of alternative services being considered, including the model of care used.
- Share with the Commissioner any information on other providers likely to be involved in the provision of care to people at the new service.
- Consider bringing forward inspection or other evaluative activities for alternative providers where only limited quality information is available (lead role).
[Note ‘share with the Commissioner’ does not have to be in writing and could be verbal or as part of any scheduled or regular meetings]
15.10.3 Local Dental Committee (LDCs)
The LDC for the area will be engaged in the following processes:
- made aware of the engagement occurring with patients
- made aware of any interim proposals and immediate next steps
- made aware of any long-term plans
This LDC section recognises that LDCs will champion the welfare of its members and wider practice staff.
15.10.4 The Process
The process for a planned practice closedown commences between 9 and 15 months prior to the scheduled end date of the contract. For unplanned closure(s), it will be necessary to undertake a rapid assessment and determine the most appropriate course of action.
In the large majority of cases where closure is rapid (i.e. immediate removal of CQC registration) the most appropriate course of action will likely involve an initial ‘caretaker’ arrangement (another dentist or dental team) temporarily overseeing the practice at the closing practice’s existing premises and the care of its patients.
15.10.5 Engagement and re-procurement
Where arrangements have been made for another dentist to temporarily manage the dental practice (refer to the chapter on Urgent Contracts), or a practice has terminated a contract with little notice (e.g. 6 month) the Commissioner should refer to the 3 stages and templates listed in this policy and guidance manual under the section above on Planned Closedown.
NHS England has several statutory duties relating to the exercise of its functions including reducing health inequalities and public involvement. The Commissioner must ensure that its actions in re-procuring a contract and any consequential actions ensure compliance with these duties. Please refer to the Chapter 2 ‘General Duties of NHS England’ for further guidance.
However, in an urgent situation, it may be necessary to balance the duty to involve with the public interest in maintaining continuity of care and protecting the health, safety and welfare of patients or staff. If a Commissioner considers acting in a way that may not comply with its statutory duties, it should seek further legal advice.
15.11 Management of Contract Hand backs
When a Contractor wishes to serve notice to hand their contract back, the Contractor should be advised to confirm all details in writing to the Commissioner. Once the letter has been received, the Commissioner should send a letter to the Contractor to confirm the termination and obtain further details on the transfer of the patient records. Please see template letter provided in Annex 15.8..
Discussions should take place with the Contractor to agree a joint letter to patients. A suggested letter is included in Annex 15.9. The letter should include alternative NHS dental practices that patients contact for treatment.
Where courses of treatment have not been completed, the Commissioner should ensure that patients are aware that where a continuation of treatment at the same or lower band within two months is needed, patients will be required to pay the relevant dental charge when this is carried out by another Contractor. Similarly, patients seeking recourse under free repair and replacement provisions need to be made aware that there will be a fee to pay if a repair and/or replacement treatment is performed by an alternative practice.
The Commissioner will need to inform their local communications team in case of media interest and inform stakeholders about the NHS services will be ceasing in the practice. This could include the local LDC and MP, Healthwatch as well as local overview and scrutiny committees. A standard statement should be agreed for any communications including where patients will be signposted too. It may be useful to establish a Communications and Engagement Plan. See Annex 15.10 for a suggested plan. Compass should be amended to show the agreed close down date so that payments cease on the agreed date and NHS.uk should be updated with the removal of the practice. The Commissioner should also update their e-mail and written distribution lists to ensure the practice is removed from the relevant lists.
15.12 Other considerations
The Commissioner may wish to undertake a needs appraisal to determine whether a contract is required in the area of the closing practice. This may result in a short-term contract being let or a procurement depending on the needs of the local area.
NHS England has a duty to inform patients regarding changes to NHS services. As part of any communication and engagement plan, the Commissioner will need to assess the needs of patients to determine whether accessible communications will be required.
Communications must consider the Accessible Information Standard which requires organisations to ensure that disabled patients receive information in formats that they can understand. For more information on the standard and guidance on its implementation see the NHS England website.
Communications must be tailored to different languages and consideration of other support for patients whose first language is not English.
16. Practice NHS.UK profiles
16.1 Introduction
Patients will often go to NHS.UK as a first point-of-call to access information around which practices nearby offer certain services, particularly whether they have NHS appointments available. It is therefore paramount to ensure that practice information available within the public scope is kept up to date and this information is accurate.
16.2 Contract requirements
Contractors are required to update or verify the information for the following modules on their NHS.UK profiles at least once every 90 days:
- opening times
- services
- facilities
- contact details
- accepting new NHS patients
At the end of each quarter Commissioners are sent an audit report containing a list of practices who have not fully updated all the modules on their NHS.UK profile. Practices who have fully updated the modules on their profile, hence meeting their contractual requirements, will not appear on the report.
Excerpt of audit report: Columns G to K provide updated status for each module.

If any of these columns contain “No” the contractors’ contractual requirements have not been met. Where there is non-compliance, the Commissioner will notify the Contractor in line with section 10 contract breaches.
Part C – General
17. Provision of occupational health services
17.1 Introduction
Occupational Health (OH) is “a specialist branch of medicine focusing on the health of staff in the workplace. OH professionals aim to find out what impact work has on staff health and make sure that staff are fit to undertake the role they are employed to do both physically and emotionally. OH specialists can support organisations through advising on work-related illnesses and accidents, carrying out assessments for new starters and existing employees, monitoring the health of employees and prevention. OH services are also used to assist organisations in managing both short and long-term absence situations” (NHS Employers).
Employers are required by law to prevent physical and mental ill health in their workers that may occur as a result their business activities. An important part of occupational health is concerned with how work and the work environment can impact on workers’ health, both physical and mental. It also includes how workers’ health can affect their ability to do their job. In health and safety law, there are things organisations must do to make sure workers’ health is not adversely affected by their work and that workers are medically fit to carry out their work safely. This includes:
- implementing health or medical surveillance when necessary, ensuring workers are medically fit to undertake the role required (your industry may produce such standards)
- reviewing your risk assessment when a worker is returning to work following sickness absence or declares a health condition
- have a responsibility to make available occupational health services for their staff and it is important that staff know how to access their service provider.” (Health and Safety Executive)
17.2 Provision of Occupational Health Services – Services funded by the primary care Contractor
This section outlines what primary care services contract holders are responsible for funding as part of their employer responsibilities to their staff. These services include:
- OH pre-employment screening/clearance: OH assessments as required for all staff working in their organisation.
- Virology testing, vaccination for blood borne viruses (BBVs) and immunisation: Available to all staff who are not already immunised, and includes Hepatitis B, Varicella, Tuberculosis (BCG), Diphtheria, Pertussis and Tetanus, Measles Mumps and Rubella.
- Enhanced/other OH assessments: This may include a range of different OH assessments or support needed for all staff including:
- Assisting in the appropriate placement of people at work, considering their physical and mental health, and prevent ill health arising as a result of work done or the conditions in which work is done
- Enhancing staff performance and morale through reducing risks at work which lead to ill health, staff absence and accidents
- Protecting the public from any adverse consequences arising because of ill health or infected primary care staff
- Reviewing prolonged/recurrent sickness absence and support return to work after sickness absence or following an accident
- Advising on ill health retirement
- Providing periodic health assessments for example: radiation, COSHH regulations or where risk assessment has indicated that this is required
- Advising on onward referral to other services that could support staff e.g. counselling.
17.3 Provision of specific Occupational Health Services – applicants to join the National Performers List
Performers seeking to apply to join the National Performers List (NPL) will need to self-fund for the following OH services: pre-employment screening, virology testing, vaccination for BBVs and immunisation.
17.4 Provision of specific Occupational Health Services – funded by the Commissioner
17.4.1 For ALL primary care staff (general practice, community pharmacy, dentistry & optometry): Management of staff on exposure to and working with BBVs
This includes specialist support for the management of staff who have a BBV, and urgent and longer-term advice to all staff working in primary care settings (including trainees) on exposure to potential BBV e.g. following needle stick injury. Post exposure risk assessments, blood testing, and post-exposure prophylaxis (PEP) treatments are included. Mainstream NHS services are responsible for ongoing treatment if BBV contracted (e.g. anti-retroviral medication).
For Performers already on the National Performers List:
OH services funded by the Commissioner include: virology testing, vaccination for BBVs and immunisation.
For Performers who are under review or investigation by Responsible Officer / Medical Director:
Any OH referrals made by Responsible Officer/Medical Director in respect of formal proceeding as part of the National Performers List.
17.4.2 Summary of ‘who pays’ for what OH services
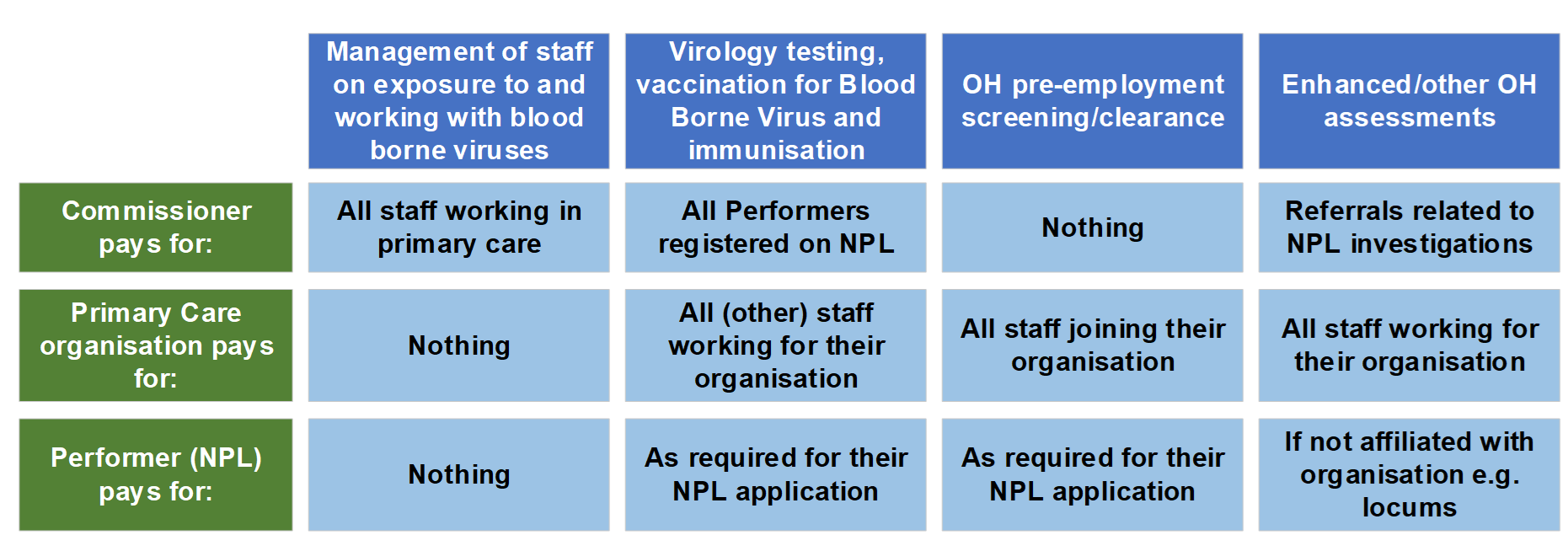
Image text:
Management of staff on exposure to and working with bloodborne viruses
- Commissioner pays for: All staff working in primary care
- Primary care organisation pays for: Nothing
- Performer (NPL) pays for: Nothing
Virology testing, vaccination for blood borne virus and Immunisation
- Commissioner pays for: All performers registered on NPL
- Primary care organisation pays for: All (other) staff working for their organisation
- Performer (NPL) pays for: As required for their NPL application
OH pre-employment screening/clearance
- Commissioner pays for: Nothing
- Primary care organisation pays for: All staff joining their organisation
- Performer (NPL) pays for: As required for their NPL application
Enhanced/other OH assessments
- Commissioner pays for: Referrals related to NPL investigations
- Primary care organisation pays for: All staff working for their organisation
- Performer (NPL) pays for: If not affiliated with organisation e.g. locums
17.5 Role of the Commissioner in enabling OH access for primary care workforce
17.5.1 Joint approach to procuring OH services:
Although the different OH provisions are a shared responsibility i.e. Commissioners fund part and primary care organisations fund part, Commissioners should take steps to support primary care staff to access OH services in a consistent and efficient way.
Commissioners are much better placed to procure system-wide OH services on behalf of primary care organisations and should enable this by procuring OH service providers for all OH requirements set out above, with the option for primary care organisations to access these OH services on a fee basis for services they are responsible for funding.
It is strongly advised that Commissioners collaborate with other primary care Commissioners (i.e. general practice, community pharmacy, dentistry, and optometry), and local NHS Organisations/ Integrated Care Boards (ICB) to ensure a cross-system sustainable and consistent access to OH services.
17.6 Good communications are essential
Commissioners must ensure information about how to access OH services are clearly communicated to primary care organisations and their staff. Many believe OH services are not available in primary care, which is not true. We must therefore do more to promote OH services available; as a minimum this should clearly present information as set out below, but Commissioners should work with their OH supplier on promotional materials and posters as required:

Image text:
Urgent occupational health services
- Management of staff on exposure to and working with bloodborne viruses e.g., needle stick injury
- Working hours: [contact [phone number / instructions]
- Out of hours: [add phone number / instructions]
Routine occupational health services
- Virology testing, vaccination for Blood Borne Virus and immunisation
- OH pre-employment screening/clearance
- Enhanced/other OH assessments
- OH provider: [supplier name]
- Website: [for more info on offer/prices]
- Phone: [supplier phone number]
- Email: [supplier email]
Publication reference: PRN01177